Posted originally on the conservative tree house on November 27, 2021 | Sundance | 172 Comments
The Times of India, a media outlet previously very skeptical of Big Pharma, is reporting from the South African Medical Association that officials are puzzled about the hype around Omicron.
The variant has only produced mild symptoms in regional patients with very little impact.
JOHANNESBURG: “The new Omicron variant of the coronavirus results in mild disease, without prominent syndromes, Angelique Coetzee, the Chairwomman of the South African Medial Association told sputnik news on Saturday.” … “We will only know this after two weeks. Yes, it is transmissible, but for now, as medical practitioners, we do not know why so much hype is being driven as we are still looking into it.” (read more)
Occam’s Razor – The new variant is being hyped because international governments need it to be hyped. The biggest threat to politicians and the global financial system attempting to Build Back Better via enlarged government spending, is not COVID; the biggest threat is anger from the citizenry over the inflation the government spending and buying of debt is creating.
What is the quickest way to eliminate the political risks due to inflation? Shut down demand. Lock down economies, turn the valves closed on economic demand and then watch price increases slow down.
Global monetary policy to maintain an economic system beneficial to Wall Street and the multinational investment class, means they need to keep interest rates low even as they print more money for Build Back Better spending and purchase their own debt. {Go Deep}
The primary way to control inflation is for central banks (ex U.S. Fed) to stop purchasing their own debt (quantitative easing) and then to raise interest rates. However, that approach would be against the interests of the legislative branch, multinational elites and international finance system (World Economic Forum agenda). As long as politicians keep spending, they must print money and buy their own debt. This causes devalued currency and inflation.
If you are a member of the political elite and you cannot stop the printing presses; and you are worried about the electoral backlash from massively rising prices hitting your citizenry; the only other way to slow inflation is to lower economic demand. How do you lower economic demand…. Omicron !!
Note that views expressed in this opinion article are the writer’s personal views and not necessarily those of TrialSite.
Free to Read and Share without paying
In our Toxicology Reports (TR) paper on COVID-19 that examined myriad issues associated with the ongoing mass inoculations (hereafter called the TR paper), we also evaluated the ratio of costs to benefits (relative to deaths) for what we termed a best-case scenario. In response to reader requests, I then performed a brief real-world cost-benefit analysis, and found the ratio of costs to benefits increased substantially compared to the best-case scenario. In this OpEd, I will start from fundamentals to show step-by-step why the ratios of costs to benefits for COVID-19 inoculations are so high in a real-world analysis, relate them to the underlying biological mechanisms that are taking place post-inoculation, and place these results in the larger context of what is being played out on a global scale.
1. WHY ARE THE RATIOS OF COSTS TO BENEFITS SO HIGH FOR COVID-19 INOCULATIONS?
First, some definitions. “Costs” are the deaths induced by the COVID-19 inoculations and “benefits” are the true COVID-19 deaths that only a “vaccine” could have prevented. Since the inoculations were given ostensibly as a preventive measure, the cost:benefit (c:b) ratio should be very low, on the order of a fraction of a percent. Also, in the remainder of this OpEd, I use the term “inoculation” mainly rather than “vaccine”, since the COVID-19 inoculants do not meet the legal definition of a vaccine (as we showed in the TR paper) or even the Patent Office definition (as we also showed in the TR paper).Subscribe to the Trialsitenews “COVID-19” ChannelNo spam – we promise
This analysis focuses on the most vulnerable 65+ demographic. Because of the high COVID-19 death rates in this demographic, the analysis would be expected to show the lowest c:b ratio for any demographic. In June/July, when we did the best-case scenario analysis for the TR paper, there were ~467,000 CDC-reported COVID-19-tagged deaths and ~2,600 VAERS-reported deaths post-inoculation (VAERS is the Vaccine Adverse Event Reporting System, and is operated jointly by the CDC and FDA). These official CDC numbers are the starting point for the present analysis.
a) Number of true COVID-19 deaths that required an inoculation for prevention
The first step in developing an actual c:b ratio is to adjust the CDC-reported COVID-19 deaths and VAERS-reported deaths to conform to real-world results.
A1) False Positives
The main diagnostic test with which patients were tagged as having COVID-19 is the real-time reverse transcription polymerase chain reaction (RT-PCR) test, hereafter called PCR test. A number of studies have shown that the false positive PCR rate is significant for COVID-19, and increases with increasing values of cycle threshold (Ct). A comprehensive assessment of the data concluded that at Ct of forty, where most of the USA testing occurred (some cases even higher), the false positives ranged from 90% to 97%. Selecting the lower part of the range (90%) reduces the number of true COVID-19 deaths that required a “vaccine” for prevention to 0.1 x 467,000, or ~47,000.
A2) Early Treatment
A number of frontline doctors have testified (and published treatment protocols as well) that ~85->95% of COVID-19-tagged cases could have been saved from hospitalization or death had their protocols been implemented at an early stage, They have testified that, instead, patients were provided treatments known to be ineffective/harmful and denied treatments known to be harmless/safe. Selecting the median of the range (90%) reduces the number of true COVID-19 deaths that required a “vaccine” for prevention to 0.1 x ~47,000, or ~4,700.
A3) Deaths attributable to COVID-19 only
For patients diagnosed with COVID-19, approximately 94% had clinically-defined comorbidities, according to the CDC. In that case, approximately 94 % of the COVID-19 deaths could have been attributed to any of the comorbidities these patients had, and only 6% of the deaths could actually be attributed to COVID-19. If pre-clinical comorbidities had been included, this number of 6% would probably be decreased further. If only 6% of the deaths could be truly attributed to COVID-19 because of absence of comorbidities, the number of true COVID-19 deaths that required a “vaccine” for prevention drops to 0.06 x ~4,700, or ~280.
As a side note, the Italian Higher Institute of Health showed “only 2.9% of the deaths registered since the end of February 2020 would be due to Covid 19”….”of the 130,468 deaths registered by official statistics at the time of preparation of the new report only 3,783 would be due to the power of the virus itself”, which is even stricter than our 6% CDC-based number.
A4) Deaths preventable by inoculation
Many studies have been performed modeling the number of COVID-19 deaths prevented by the inoculations. The most conservative of these studies showed that for Sao Paolo, Brazil “almost 170 thousand deaths…..will occur by the end of 2021 for Sao Paulo…..If in contrast, Sao Paulo…..had enough vaccine supply and so started a vaccination campaign in January with the maximum vaccination rate, compliance and efficacy, they could have averted more than 112 thousand deaths”. This extremely conservative estimate reduces the number of true COVID-19 deaths that required a “vaccine” for prevention to 2/3 x ~280, or ~190!
Thus, the number of true COVID-19 deaths that required a “vaccine” for prevention was about 0.04 percent of the number of COVID-19 deaths reported by the CDC! Except for A4, the first three issues (A1-A3) were known in 2020, well before the rollout of the mass inoculations. In other words, the benefit possible from mass inoculation was exceedingly small, and did not justify mass inoculation of hundreds of millions of people in the USA with an inadequately tested new technology “vaccine”. This small potential benefit almost ensures that any c:b ratio will be relatively large, given even a moderate number of deaths resulting from the inoculation.
b) Number of actual deaths resulting from the mass inoculations
At this point in the analysis, with no scale-up from deaths reported to VAERS, the actual c:b ratio is ~870/190, or ~4.6. However, many studies have shown that the VAERS deaths are under-reported substantially. The Harvard Pilgrim Health Care tracking study showed “fewer than 1% of vaccine adverse events are reported”, similar to some of our results in the TR paper. Jessica Rose showed that the number of deaths is underreported by a factor of 31, and Steve Kirsch showed that the deaths are underreported by a factor of 41. Using the lowest of these estimates (31), the c:b ratio skyrockets to ~143, while the number of deaths is relatively modest at 870 x 31, or ~27,000. The c:b ratio for this case is about five orders of magnitude above the desired target for a “vaccine” or vaccine-proxy, as was stated at the beginning of this OpEd. Even if some of the selected parameters could be relaxed downwards, it is difficult to see where much more than perhaps an order of magnitude reduction in c:b ratio could be obtained.
While c:b ratios on the order of hundreds have not been shown by previous c:b analyses (especially for the most vulnerable 65+ demographic), and may seem extreme at first glance, they reflect the underlying reality. The only reason they do seem extreme is that the political and biomedical media have framed the narrative that these inoculations are safe and effective, with the implication that their c:b ratios are extremely low. As I have shown above, only a very small cadre of individuals could have benefited potentially from these inoculations. Mass inoculations of hundreds of millions of people in the USA with an unproven technology produced damage that overwhelmed any small potential benefits.
It should be re-emphasized that this conservative analysis was for the most vulnerable 65+ demographic. As we proceed to lower age demographics, we can expect the c:b ratios to go substantially higher, since deaths of COVID-19-tagged individuals decrease drastically with decreasing age. Also, these numbers reflect very-short-term results only, and the hands-on results of Drs. Hoffe, Cole, and others showing alarming values of Early Warning Indicators do not bode well for increased “vaccine-induced” deaths even in the mid-term, with the attendant increase in c:b ratios.
2. WHAT ARE THE BIOLOGICAL MECHANISMS THAT UNDERLIE THESE HIGH COST/BENEFIT RATIOS?
The results of a realistic cost-benefit analysis should reflect the underlying technical performance of the technology being evaluated. What are the features of the inoculant being analyzed that account for its extraordinary high c:b ratios?
First, there are at least three types of toxicities associated with the inoculant. The spike protein resulting from the inoculant is extremely toxic, as shown in detail in the TR paper. The LNP encapsulating shell has some extremely toxic components, such as polyethylene glycol, to which many people are sensitive (also as shown in the TR paper) and cationic lipids. The desired product of the inoculations, anti-spike protein antibodies, can react with tissues and cause myriad types of damage.
Second, it evades the immune system in two ways. It is injected, thereby entering the bloodstream directly and indirectly, and by-passing that part of the innate immune system that inhaled viruses encounter initially. The LNP-encapsulating shell, which provides mRNA stability, was developed initially for drug delivery and similar applications, where the target is to deliver drugs to any tissue or organ in the body. In this case, increased time spent in the circulatory system is the goal. For the present application, long residence time in the circulatory system means that the vascular damage and clotting associated with the spike protein endocytic merging with the endothelial cells can occur throughout the body. This impact is seen in the types of damage listed in VAERS, and in post-inoculation autopsies. Third, while it boosts the antibody titers for a few months, it affects the immune system adversely.
Are there any positive benefits from the inoculations? Obviously, increasing antibody titers against the relevant viral strain will offer some protection before waning immunity commences. For some elderly who are concerned with short-term survival there could be benefits. The inoculation also reduces the severity of symptoms for some people. Because appropriate treatments were withheld from numerous patients, the inoculations saved lives that would have been saved had the proper treatments been administered. But the benefits under the condition that appropriate treatments were administered were small relative to the adverse effects from mass inoculation.
3. HOW DO THESE RESULTS FIT WITHIN THE LARGER PICTURE OF GLOBAL MASS INOCULATIONS AND MANDATES?
The following appears to be the larger picture encompassing the details presented above. In December 2019, a viral outbreak appeared to occur initially in Wuhan, China. There is not consensus on its origins, but it appears the virus was engineered in a lab and released either deliberately or accidentally. It also appears that the outbreak transitioned rapidly into a pandemic. In order for the latter to occur, at least two conditions were required: rapid growth of infections globally, and substantial numbers of deaths from the infection.
A PCR test conducted at high Ct values giving very high numbers of false positives satisfied the rapid growth of infections requirement. COVID-19-tagged patients denied appropriate treatments and given ineffective treatments satisfied the requirement of substantial numbers of deaths from the infection. According to Drs. Zelenko and Ardis, and many others who developed successful treatment protocols for COVID-19-tagged patients, most of the COVID-19-tagged patients could have been saved had the protocols been applied early. Most people who were COVID-19-tagged and died had their deaths attributed to COVID-19. The withholding of appropriate treatments had a double benefit to enforce pandemic measures; it also meant that an EUA could be issued for a “vaccine”, since no alternative treatments were available.
After a few short months of clinical trials, the EUA was granted, and mass inoculations were started in mid-December 2020, about one year after the outbreak occurred. This meant that the inoculants were developed and tested within one year, a process that ordinarily takes 12-15 years. As shown in the TR paper, the clinical trials were questionable, and no long-term testing was done.
The mass inoculations in the USA have been ongoing for about ten months, and almost 200 million people have been fully vaccinated. VAERS reports a fraction of the very-near-term adverse effects, but actual scaled-up numbers are mainly estimated. While the elderly, especially with comorbidities, seem to experience the most deaths, children who previously showed no signs of illness are experiencing large numbers of serious effects such as myocarditis. Early warning indicators, such as high D-dimer and troponin levels after inoculation, are an ominous sign of future problems. Steve Kirsch has summarized many of these demonstrated and future adverse effects in an excellent slide presentation.
Dr. Ryan Cole, CEO of a large independent diagnostics lab in Idaho, states in many videos that he has been seeing a twenty-fold increase in uterine cancer since inoculations began. Dr. Byram Bridle states the following cancer prediction succinctly: “What I have seen way too much of and it does cause me very serious concern is that we are seeing people who had cancers that were in remission or that were being well controlled and their cancers have gone completely out of control after getting the vaccine. We do know that the vaccine causes at least a temporary drop in T-Cell numbers. T-Cells are part of our immune system and they are the critical weapons that our immune system has to fight off cancer cells.” Numerous doctors are starting to report anecdotes of increased cancer, although these effects have not yet been documented in the biomedical literature.
Studies from the UK and Sweden, among many others, seem to indicate that the second mRNA dose confers immunity for about six months, after which a booster is required to maintain immunity. This could mean that boosters would be required every six months (or sooner) indefinitely, and each booster would be accompanied by adverse effects (such as the micro-clotting that Dr. Hoffe has reported in his patients). If these effects are cumulative and irreversible, that would spell disaster for those on the endless treadmill of booster—short-term immunity—waning immunity—possible negative effectiveness—booster…..
Beneficiaries from the lockdowns, restrictions, and mass inoculations appear to be 1) the governments worldwide who increased control over their people and implemented vaccine passports to different degrees; 2) the companies who manufacture the inoculants and drugs that will be needed to address the many adverse health effects resulting from the inoculations and boosters; and 3) the organizations who specialize in online and remote business operations, such as the Big Tech companies. Whether any of these beneficiaries played a major role in the events remains to be seen (and decided in courts of law).
It is unclear why the five major stakeholders (healthcare industry, government at all levels, mainstream media, medical profession, academia) involved in promoting the restrictions and mass inoculations are reading from the same sheet of music. While the government is “captured” by industry and does its bidding, and the other three stakeholders are effectively “captured” by industry (and its proxy the government) because of the funding they receive from industry and government, it is unclear why all these stakeholders would have the same attitude when it comes to harming segments of the American population through e.g., mass inoculation with unproven safety.
In particular, why would the Presidents of Universities and Principals of secondary schools, who have “in loco parentis” responsibilities for the students in their charge, be willing to sacrifice the health of their students just to maintain their research funding or salaries? These “leaders” know full well that their charges are not at risk from COVID-19, but are at substantial risks from the demonstrated adverse effects of the inoculants, and potential future adverse effects. Yet, except for a few isolated instances, there is no action taken to refuse these mandates and protect their charges; rather, action is taken to double-down on the mandates!
The five major stakeholders’ actions to inoculate the full population of the USA in particular have resulted/are resulting/will result in physically, economically, strategically destroying the USA as a sovereign power and world leader. They are producing a populace that is becoming physically addicted to the inoculations and requisite boosters, and is becoming more subservient to a government that mandates these inoculations as a condition to access all that a civilized society has to offer. By the end of 2021, all those who operate the critical USA infrastructure (e.g., police, firefighters, military, healthcare professionals, teachers, pilots, etc.) will have been inoculated by mandate, and the non-compliers will be terminated from their jobs. If our projections of future adverse effects are correct, those who have been inoculated will be at higher risk for damage, and when the symptoms emerge after a lag period, the USA will be functionally paralyzed.
In stark contrast, our research group has been producing monographs and journal papers showing that severe reactions to the viral exposure are the result of a dysfunctional immune system, that this dysfunction is mainly caused by exposure to toxic stimuli and adoption of toxic behaviors, and these severe reactions can be prevented by identifying and removing these toxic contributing factors as broadly, deeply, and rapidly as possible. One bonus of the latter is that many of the comorbidities that accompany COVID-19 serious effects will be eliminated as well.
In summary, the COVID-19 inoculations are not justified from any cost-benefit perspective. The potential benefits are too small to justify mass inoculations with their demonstrated large numbers of very-short-term adverse effects, and potential ADE, autoimmune, neurological, cancer, etc. adverse effects in the mid-and long-terms. The above holds true even for the most vulnerable (elderly with many comorbidities) and is especially true for the least vulnerable from COVID-19, the children who may have to bear the brunt of adverse effects potentially for the rest of their lives.
If those at high/medium risk from COVID-19 want to take the inoculation, that should be a decision between them and their doctor. It should not be mandated, and restrictions should be lifted immediately.
Note that views expressed in this opinion article are the writer’s personal views and not necessarily those of TrialSite.
Dr. Ron Brown – Opinion Editorial
November 26, 2021
No one should be surprised that the world is anxiously overreacting to news of the latest coronavirus variant B.1.1.529: WHO meets amid global alarm over new Covid-19 variant. After all, the public has been conditioned to overreact to the discovery of “novel” coronaviruses” during the COVID-19 pandemic by none other than the master disinformation disseminator himself, Dr. Anthony S. Fauci: ‘If it looks like you’re overreacting, you’re probably doing the right thing’. Fauci’s misinformed advice has encouraged hasty, counterproductive, and damaging public health decisions based on surveillance data falling directly into the hands of anxious public health authorities—before being vetted and interpreted by more thorough epidemiological analyses to determine actual virus severity and spread. Consequently, the hysterical public health message implied through the media is that there is no time for all that if we are all dead!
So what is Dr. Fauci’s advice so far on B.1.1.529? What Fauci Said About B.1.1.5…Quality journalism costs money to produce. We will be reinvesting the proceeds of these subscriptions into an increasing volume of high quality, independent, unbiased reporting and expert analysis. Our subscription tiers use the ‘honor system’ – please do not abuse it. All tiers of service provide the same level of access to content. We are grateful for all of you, and we hope you reciprocate.
Note: If you need assistance with your subscription or would like to discuss a corporate subscription for more than 10 employees please contact us or use the chat (bottom right).
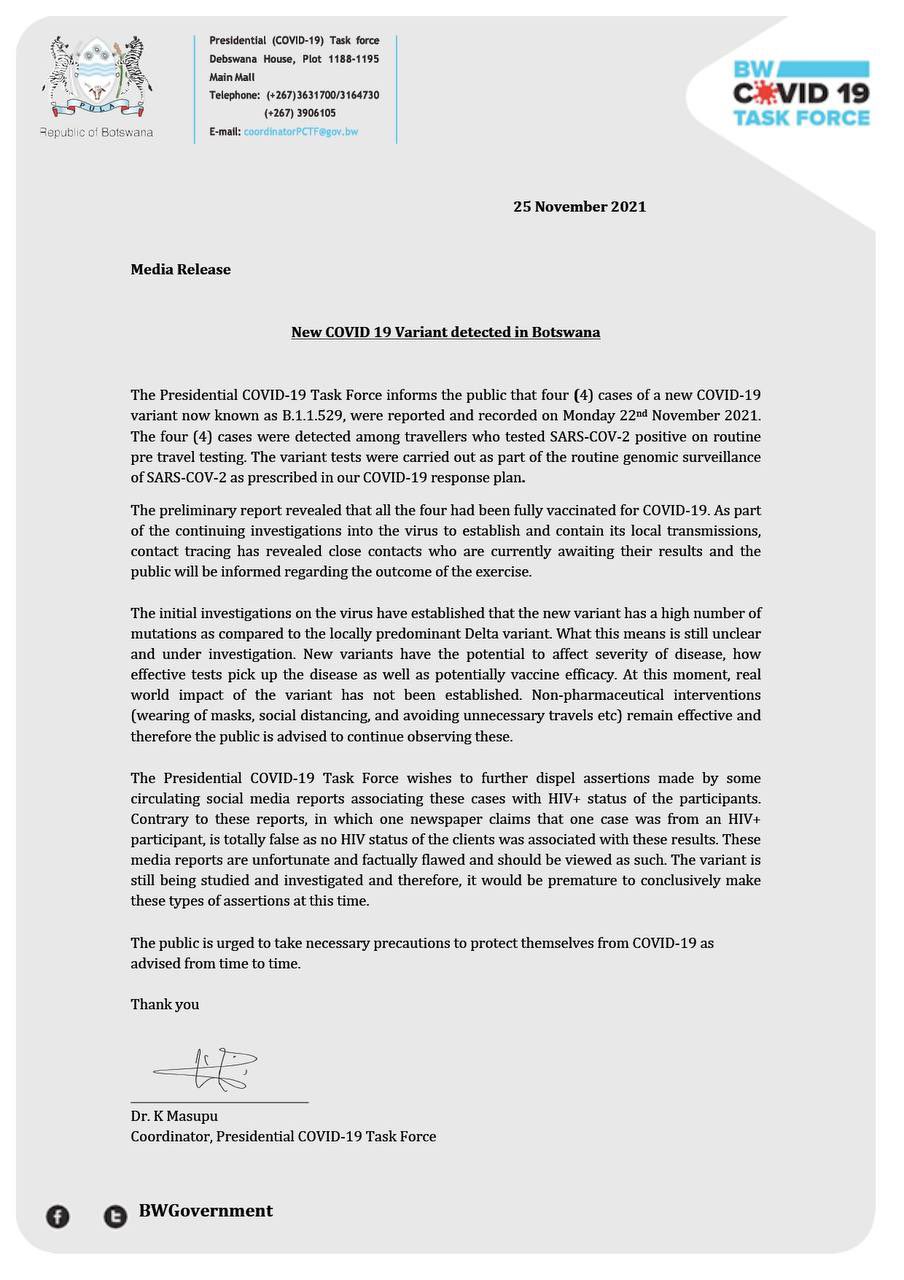
On November 25, the Botswanan COVID-19 Task Force reported four new cases of the COVID variant B.1.1.529. All four cases were detected in travelers through routine PCR testing. They noted something interesting about all four cases:
“The preliminary report revealed that all four had been fully vaccinated for COVID-19.”
Yes, all four individuals with detectable cases of B.1.1.529 were fully vaccinated. There have been numerous breakthrough cases of COVID-19 and the Delta variant among the vaccinated. Now, it appears that those who have taken the vaccine may be more susceptible to transmission as this new variant is associated with increased antibody resistance. The report states that they are uncertain if the currently available vaccinations will prevent transmission and suggests “non-pharmaceutical interventions,” such as masks, social distancing, and avoiding unnecessary travel. Governments now have a new reason to reimplement harsh restrictions. The upcoming days and weeks should shine a light on what they plan to do to “stop the spread” since the vaccine is not as “safe and effective” as previously claimed.
The Dow experienced its steepest decline of the year on Friday after it was reported that the COVID-19 virus mutated into a variant called B.1.1.529. Virologists and immunologists are extremely concerned by the number of strains this virus carries, with over 32 detected so far. The National Institute for Communicable Diseases (NICD) has confirmed 22 cases of the virus in South Africa. At the time of this writing, numerous countries such as Italy, France, the UK, and Singapore have banned flights from South Africa and other African nations. Once cases are detected in other countries, we will likely see a further increase in travel bans and restrictions. This news comes weeks after many nations reopened their borders for travel.
Scientists do not understand the variant or strains yet and claim more data is needed. Health agencies are now scrambling to determine the next steps. It is also unknown whether the currently available vaccinations will protect anyone against B.1.1.529, but it has been reported that the strain will spread faster than the Delta variant. The new mutation has increased antibody resistance, which may lead one to believe that the “experts” will push for a new vaccine or booster. If this virus spreads as rapidly as claimed, then we should expect increased government restrictions. They’ve already locked down the world once, destroyed the economy, and they could do it again.
Posted originally on the conservative tree house on November 26, 2021 | Sundance | 203 Comments
Wow, 72 hours ago no one even heard the name Omicron variant. Now, in less than three days, a variant has been identified, global travel has been halted, states of emergency have been declared, and now we see a pharmaceutical company announcing the variant specific vaccine trial that will begin in the U.S. in a few weeks. This government relationship with Big Pharma is certainly generating some fast action, eh?
If a person was cynically inclined; while knowing governments’ need to control inflation yet cannot raise interest rates or stop purchasing debt because current legislative spending continues – a remarkable control option would be to halt demand; and a person might think this was suspicious, or something.
Nov 26 (Reuters) – Novavax Inc said on Friday it had started working on a version of its COVID-19 vaccine to target the variant detected in South Africa and would have the shot ready for testing and manufacturing in the next few weeks.
The company’s COVID-19 shot contains an actual version of the virus’ spike protein that cannot cause disease but can trigger the immune system. The vaccine developer said it had started developing a spike protein specifically based on the known genetic sequence of the variant, B.1.1.529.
Novavax’s vaccine received its first emergency use approval earlier this month in Indonesia followed by the Philippines. Other vaccine developers, including Germany’s BioNTech SE and Johnson & Johnson, have said they are testing the effectiveness of their shots against the new variant, which is named Omicron by the World Health Organization (read more)
Posted originally on the conservative tree house on November 26, 2021 | Sundance | 268 Comments
All the totalitarians will quickly follow suit. New York Governor Kathy Hochul declares a state of emergency, granting herself additional power and authority as the threat of Omicron is utilized. They are moving fast on this one; no time to waste. How long before new lockdowns? Keep watching…
New York – New York Gov. Kathy Hochul issued a state of emergency order on Friday in response to the identification of the COVID-19 omicron variant.
The emergency order is intended to increase hospital capacity in New York and will last until at least Jan. 15, when it will be reassessed.
According to a copy of the order, the state will utilize the “surge and flex system,” which allows the Department of Health to limit non-essential and non-urgent hospital procedures in situations where a hospital has less than 10% staffed bed capacity. (read more)
Place your bets… who will be next? Newsom, Whitmer or other?
Posted originally on the conservative tree house on November 26, 2021 | Sundance | 65 Comments
According to sources familiar with the matter, who wish to remain anonymous as they are not authorized to relay information from two other anonymous officials with knowledge of a person once seen next door to an official who directly overheard a conversation relayed by several officials at the heart of the issue, there might be a coded message here.
Joe Biden and Kamala Harris are banning African travelers on Black Friday 2021:
A congressional investigation surrounding this blatant air travel discrimination is warranted. How is it fair a person of color who walks across the U.S. border can be protected by COVID immigration policy, yet an African person of color flying into the country is given no due process? Racism, gottabe. Impeach!
In order for leftists to continue advancing their insane communist ideology they must pretend not to know things:
Posted originally on the conservative tree house on November 26, 2021 | Sundance | 426 Comments
We originally outlined the new COVID-19 variant along with the international motives of the science community for delivering it HERE. Previously the new worrisome, 10 spike, vaccine resistant variant was called “The B.1.1.529 variant“. However, those types of names do not work well for larger fear narrative distribution. As a result, the international scientific community has given it the name “Omicron“. Perhaps the “Merry Christmas” variant would be culturally insensitive.
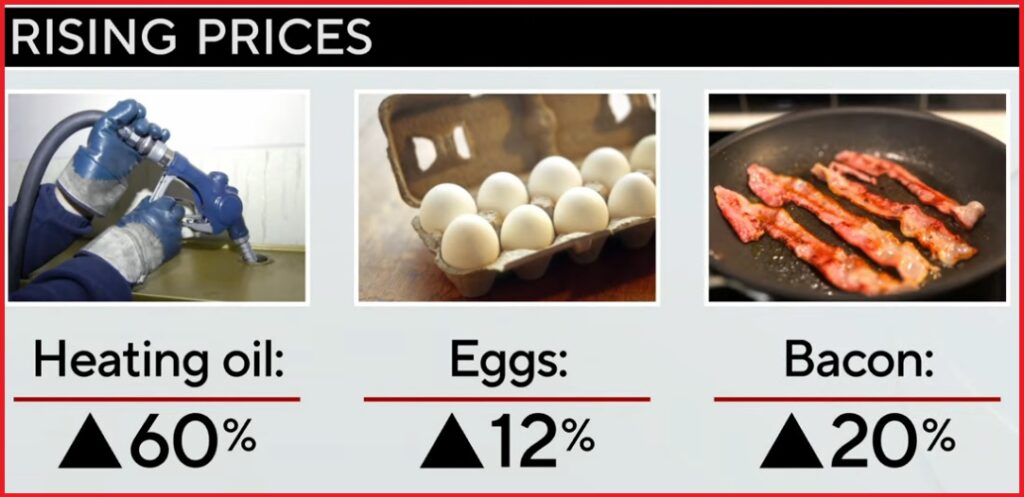
Globally, and not coincidentally –politically– the greatest challenge to those in power is a massive rise in direct inflation. What is the quickest way to eliminate the political risks due to inflation? Shut down demand….. lock down the economies… turn the values closed on economic activity, and then watch oil prices plummet.
As the science is told, Omicron originated in South Africa, Botswana, Zimbabwe, Namibia, Lesotho, Eswatini, Mozambique and Malawi. Government officials around the world have responded to the Omicron variant by banning travel from those countries. The U.K and Australia kicked off the latest round of fear porn with their travel bans. Subsequently, fellow EU nations Austria, France, Italy, the Netherlands and Malta all announced imminent entry bans to all travelers who’ve entered South Africa and surrounding nations in the past two weeks.
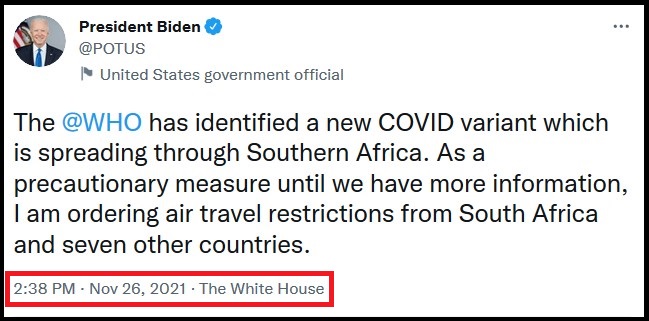
In North America, Canada will be “banning the entry of foreign nationals…that have traveled through southern Africa in the last 14 days,” due to the new coronavirus variant Omicron, Health Minister Jean-Yves Duclos said at a news conference Friday. (link) And right on cue the Biden administration joins the effort:
WHITE HOUSE – “This morning I was briefed by my chief medical advisor, Dr. Tony Fauci, and the members of our COVID response team, about the Omicron variant, which is spreading through Southern Africa. As a precautionary measure until we have more information, I am ordering additional air travel restrictions from South Africa and seven other countries. These new restrictions will take effect on November 29. As we move forward, we will continue to be guided by what the science and my medical team advises.” (more)
The discovery of a new Covid-19 variant sent oil plummeting 13% on Friday, as investors feared a wave of new government restrictions and slower economic growth.
US crude finished the day at a two-month low of $68.15 a barrel, down 13.1% from Wednesday’s close. It was the worst day for oil since April 27, 2020, when Covid was spreading rapidly in the US. (link)
Under this type of economic manipulation using science, the U.S. federal government -and the multinational governments as a whole- recapture control of inflation.
As you know, the monetary policy to maintain an economic system beneficial to Wall Street and the multinational investment class means they need to keep interest rates low even as they print more money vis-a-vis the Build Back Better spending operation. {Go Deep} The primary way to control inflation is for central banks (U.S. Fed) to stop purchasing their own debt and/or raise interest rates. However, that approach would be against the interests of the multinational elites and international finance system (World Economic Forum agenda).
If you are a member of the political elite and worried about the electoral backlash from massively rising prices hitting your citizenry….. Another way to stop inflation is to shut down economic demand.
How do you shut down global economic demand…. Omicron !!
See how that works?
As a result, we enter the 2022 mid-term election under a scenario where a new variant of COVID, Omicron, is now the reason for government rules (Vaxx, Vaxx, Vaxx), a slowed economy and a contraction of demand. Omicron becomes a justification and excuse for lowered economic expectations.
Simultaneously, inflation is artificially paused by using Omicron as a pressure valve, and the central bankers don’t have to worry about negative consequences to the multinational corporations who give them instructions.
Under this strategy, the electorate can be duped into reinstalling political ideologues, elites and communists. And guess what? The U.S. Energy Secretary doesn’t need to know what the price of a barrel of oil costs.
Don’t blame me, we just see this COVID variant stuff for what it is…. useful.
This ain’t their first rodeo.
It’s not clear yet whether the mutations make this variant more infectious or whether it causes more severe illness, but researchers say the high number of mutations to the “spike proteins” — the focus of a body’s immune response — may make it more able to get past the body’s defenses. (link)
A VICE News special shows how the pharmaceutical companies lobby the Food and Drug Administration (FDA) to approve dangerous drugs. This is not a new revelation, but most blindly trust the FDA stamp of approval. Big Pharma currently spends over $4.5 billion on lobbying efforts to approve their drugs. For example, in 1995 Purdue produced the notoriously addictive drug Oxycontin. Reports stated that less than 1% of those who took the drug would become addicted. Since then, over 500,000 million Americans have died from the narcotic. Purdue has since faced numerous lawsuits and intense scrutiny; however, the FDA has escaped any blame.
More recently, the FDA approved the Alzheimer’s drug Aduhelm by Biogen after clinical studies showed that the drug did not work. The drug, which costs $56,000 annually, was originally denied by regulators. Then the lobbyist entered and essentially paid the FDA to pass the drug. Let’s not forget, once a drug is FDA approved, the pharmaceutical company is permitted to advertise. Hence, why Pfizer began to produce commercial, radio, and print advertisements within the same week of receiving FDA approval this year.
(Six pairs of prosthetic limbs made for Tracey Baynam, whose limb development was affected by thalidomide, throughout her childhood and teenage years. Science Museum Group)
The greed of the FDA knows no bounds. FDA Dr. Kelsey singlehandedly saved millions of Americans in the 50s and 60s from a dangerous drug called Thalidomide. The drug was originally prescribed to pregnant women to reduce morning sickness. Thousands of children across the world were born with serious birth defects due to Thalidomide. The lifelong debilitating outcome of the drug prompted harsher drug testing worldwide, in theory. Unsurprisingly, Thalidomide is still available with a prescription. A regulator’s approval has never meant that a drug was safe for use. The FDA is bought and paid for by Big Pharma, and truth be told, they do not know the long-term side effects of the new medications they are approving.
I have created this site to help people have fun in the kitchen. I write about enjoying life both in and out of my kitchen. Life is short! Make the most of it and enjoy!
This is a library of News Events not reported by the Main Stream Media documenting & connecting the dots on How the Obama Marxist Liberal agenda is destroying America