Acclaimed vaccinologist, Geert Vanden Bossche, sits down for his second groundbreaking interview with Del to explain why the intense pressure mass vaccination is putting on the Covid-19 virus will likely drive it to become catastrophically deadly. Click on the arrow on the right side of the image to watch.
Posted Originally on the conservative tree house on April 20, 2022 | Sundance
Put this in the tab labeled ‘conclusive proof of prior suspicions.’
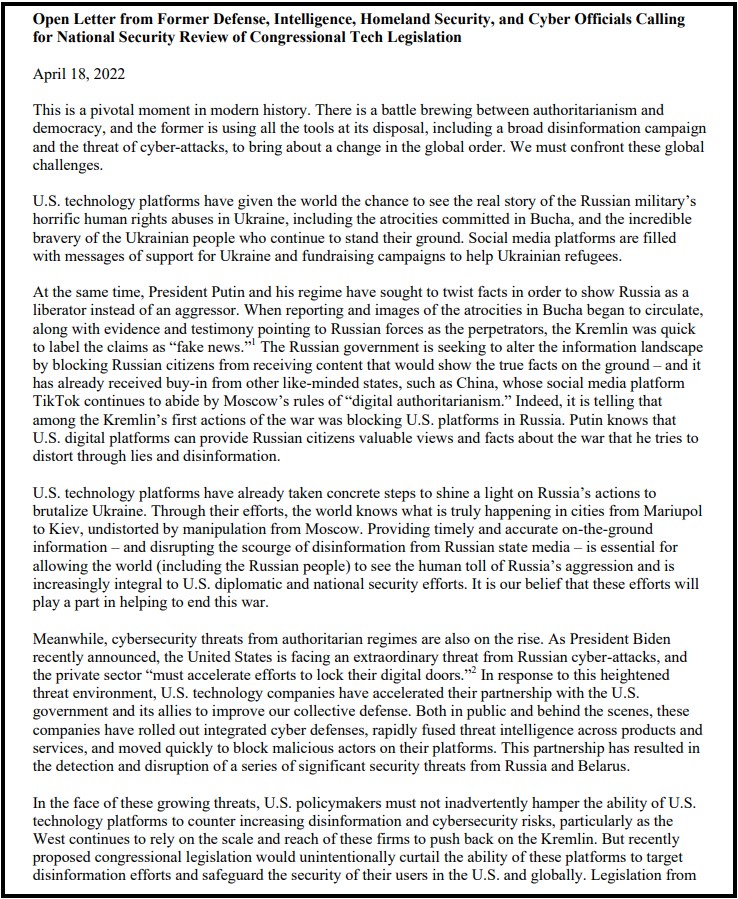
Former Obama era intelligence officials, those who helped construct, organize and assemble the public-private partnership between intelligence data networks and supported social media companies, have written a letter to congress warning that any effort to break up Big Tech (Twitter, Facebook, Instagram, Google, Microsoft, etc.) would be catastrophic for the national security system they have created.
Citing the information control mechanisms they assembled, vis-a-vis the ability of social media networks to control and approve what is available for the public to read and review, the intelligence officials declare that any effort to break up the private side of the intel/tech partnership will only result in less ability of the intelligence apparatus to control public opinion.
They willfully admit that open and uncensored information is adverse to the interests of the intelligence state and therefore too dangerous to permit. They specifically argue, if the modern system created by the partnership between the U.S. government and Big Tech is not retained, the national security of the United States is compromised. Let that sink in for a moment.
One of their reference citations revolves around Ukraine and the Russia narrative:
“U.S. technology platforms have given the world the chance to see the real story of the Russian military’s horrific human rights abuses in Ukraine, including the atrocities committed in Bucha, and the incredible bravery of the Ukrainian people who continue to stand their ground. Social media platforms are filled with messages of support for Ukraine and fundraising campaigns to help Ukrainian refugees.” (Paragraph 2, Letter)
Keep in mind the “Bucha” narrative is widely disputed by people who have reviewed the western government/media evidence.
There is equal evidence the Bucha narrative was a western intelligence operation, created to give a false impression and generate public support for advanced military operations in Ukraine.
Seeing this public relations effort using the Bucha story as evidence to support their goal of keeping Big Tech isolated from legislative review, only lends more credence to suspicions the Bucha events were a U.S. led intelligence operation (false flag).
Glenn Greenwald has a good take on the granular details behind their letter:
[…] This is where these former intelligence and national security officials come in. While these former CIA, Homeland Security and Pentagon operatives have little sway in the Senate Judiciary and House Antitrust Committees, they command great loyalty from Congressional national security committees. Those committees, created to exert oversight of the U.S. intelligence and military agencies, are notoriously captive to the U.S. National Security State.
The ostensible purpose of this new letter is to insist that Big Tech monopoly power is vital to U.S. national security — because it is necessary for them to censor “disinformation” from the internet, especially now with the grave Russian threat reflected by the war in Ukraine — and they thus demand that the anti-Big-Tech bills first be reviewed not only by the Judiciary and Antitrust Committees, but also the national security committees where they wield power and influence”… (read more)
Of course, the Fourth Branch of Government would want to get the Senate Select Committee on Intelligence involved. The SSCI created all of the mechanisms to facilitate the existence of the Fourth Branch of Government. However, I would take the issue deeper…. and ask readers to see what really worries the intelligence apparatus about the potential breakup of Big Tech.
These are the intelligence people who constructed the model for Jack’s Magic Coffee Shop.
This public-private partnership between the cyber division of the intelligence apparatus and Big Tech social media is where the free coffee comes from.
Twitter, Facebook, Instagram, YouTube and even Google itself, are financially and operationally dependent on the scale of the data processing system that is run by the U.S. government. The capacity of each of the big social media companies to exist, operate and be financially viable, is dependent on the backbone of interconnected data networking, and massive data processing.
The scale of simultaneous user data-processing is not financially viable without the U.S government subsidizing it. That’s the free coffee that cannot be duplicated in the private sector by any competing social media company. That’s the cost and scale system behind the partnership that permits Big Tech to operate. Ultimately, this is what the intelligence apparatus needs to keep hidden from the American (and global) public.
The biggest of the Big DATA processing is done through a public-private collaboration between Big Tech and Big Government/Intel.
Any private sector entity who attempts to create, or duplicate the scale of social media runs into this cost issue. It is just too expensive to operate a competing coffee shop without the free coffee. That’s why the coffee providers are lined up against Elon Musk’s attempt to buy Twitter.
The ramifications of the public discovering Facebook and Twitter social media are only possible with subsidy from government tech architecture are massive. Essentially, the U.S. government is in control of our social media networking. That’s the bigger story behind this letter.
These officials are trying to preserve the surveillance system they created.
The public-private partnership is a system for surveillance of the American people through technology.
BACKGROUND – The volume of metadata captured by the NSA has always been a problem because of the filters needed to make the targeting useful. There is a lot of noise in collecting all data that makes the parts you really want to identify more difficult to capture. This admission, along with the admission of collaboration from 2021, puts a social media filtration system in the metadata that circumvents any privacy protections for individuals.
Previously, the Intelligence Branch worked around the constitutional and unlawful search issue by using resources that were not in the United States. A domestic U.S. agency, working on behalf of the U.S. government, cannot listen on your calls without a warrant. However, if the U.S. agency sub-contracts to say a Canadian group, or foreign ally, the privacy invasion is no longer legally restricted by U.S. law.
What was announced in June 2021 was an admission of a relationship with Big Tech along with open intent to define their domestic political opposition as extremists.
July 26, 2021, (Reuters) – A counterterrorism organization formed by some of the biggest U.S. tech companies including Facebook (FB.O) and Microsoft (MSFT.O) is significantly expanding the types of extremist content shared between firms in a key database, aiming to crack down on material from white supremacists and far-right militias, the group told Reuters.
Until now, the Global Internet Forum to Counter Terrorism’s (GIFCT) database has focused on videos and images from terrorist groups on a United Nations list and so has largely consisted of content from Islamist extremist organizations such as Islamic State, al Qaeda and the Taliban.
Over the next few months, the group will add attacker manifestos – often shared by sympathizers after white supremacist violence – and other publications and links flagged by U.N. initiative Tech Against Terrorism. It will use lists from intelligence-sharing group Five Eyes, adding URLs and PDFs from more groups, including the Proud Boys, the Three Percenters and neo-Nazis.
The firms, which include Twitter (TWTR.N) and Alphabet Inc’s (GOOGL.O) YouTube, share “hashes,” unique numerical representations of original pieces of content that have been removed from their services. Other platforms use these to identify the same content on their own sites in order to review or remove it. (read more)
The influence of the Intelligence Branch now reaches into our lives, our personal lives through their efforts in social media.
In the decades before 9/11/01 the intelligence apparatus intersected with government, influenced government, and undoubtedly controlled many institutions with it. Back then, the legislative oversight function was weak and growing weaker, but it still existed and could have been used to keep the IC in check. However, after the events of 9/11/01, the short-sighted legislative reactions opened the door to allow the surveillance state to weaponize.
After the Patriot Act was triggered, not coincidentally only six weeks after 9/11, a slow and dangerous fuse was lit that ends with the intelligence apparatus being granted a massive amount of power. The problem with assembled power is always what happens when a Machiavellian network takes control over that power and begins the process to weaponize the tools for their own malicious benefit. That is exactly what the installation of Barack Obama was all about.
The Obama era intelligence team took pre-assembled intelligence weapons we should never have allowed to be created and turned those weapons into tools for radical, political and fundamental change. The target was the essential fabric of our nation. Ultimately, this corrupt political process gave power to create the Fourth Branch of Government, the Intelligence Branch. From that perspective, the fundamental change was successful.
[…] “The vision was first outlined in the Intelligence Community Information Technology Enterprise plan championed by Director of National Intelligence James Clapper and IC Chief Information Officer Al Tarasiuk almost three years ago.” … “It is difficult to underestimate the cloud contract’s importance. In a recent public appearance, CIA Chief Information Officer Douglas Wolfe called it “one of the most important technology procurements in recent history,” with ramifications far outside the realm of technology.” (READ MORE)
One job…. “take the preexisting system and retool it so the weapons of government only targeted one side of the political continuum.”
Posted originally on the conservative tree house on January 23, 2022 | Sundance | 146 Comments
Earlier today tens of thousands of people, vaccinated and unvaccinated, attended the “Defeat The Mandates” rally in Washington DC. Among the notable speakers was Dr. Robert Malone {Direct Rumble Link} and Robert Kennedy Jr. {Direct Rumble Link}.
A band new system of governance has been created over the past two years, as the pandemic of SARS-COV-2 ravaged the world; and I’ll call this new system Fauciism, What follows next is the logic for creating this new word.
Starting long before the emergence of the VOVID-19 virus in Wuhan China in November/December 2019 Anthony Fauci MD was hard at work plotting his new idea on Technocratic rule over the masses. For those not familiar of the Technocratic system one must go back to the 1920’s in America and you will find a movement associated with Columbia University in New York city, that took hold after the 1929 mark crash. The movement was centered in the principle of the best and the brightest meaning scientists and engineers should be the ones to rule the world. The goal was to optimize economics to the highest possible efficiency.
Patrick M. Woods in his book Technocracy Rising gives an excellent summary of the attempted takeover of the entire world by those that believe they were destined to rule us all. This is a very real movement and that book is a must read as it connects a lot of dots. So what we have in Anthony Fauci is the use of medical technology by him to create fear that can then be used to control the masses.
Robert F, Kennedy Jr. has written a definitive book on the evils that Anthony Fauci has done called The Real Anthony Fauci and after the first chapter you will understand why I am writing this.
The process is called Mass Psychosis in which a large segment of a society is conditioned by the use of fear e.g. the COVID-19 and the exaggerated high probability that you will die if you catch it. To avoid dying the citizens are told that they must do certain things. That results in a Totalitarianism form of government. This process was used to great success by Hitler and Stalin and resulted in WW II. There are three books that should be read; the first is The Origins of Totalitarianism by Hannah Arendt, the second in The Gulag ArchipelagoVol I by Aleksandr Solzhenitsyn and the third is Obedience to Authority by Stanley Milgram.
If you read these books, you will understand exactly what is happening in Western civilization today. However, it’s hard to read all of the Gulag as what is described is unpleasant so only read what you can take. The point is that unless we break free of the fear the Gulag explains how in will end.
Fauci is not the one funding this abomination that honor belongs to Bill Gates. And the other one that takes advantage of the fear is Klaus Schwab the creator of the World Economic Forum (WEF) that wants to rule the world. But neither Gate nor Schwab could have pulled this off without Fauci so he is the one that must be given the credit for creating this new system of the tyranny of the Medical system hence forth Fauciism. This system of Fauci is responsible for killing between 70% and 80% of the COVID worldwide deaths and since those deaths aren’t over, he could easily be the holder of the world record in a few more years. The following figures were taken from Our World Data (Oxford University) on January 21, 2022, using 75% preventable. Note: the 70% & 80% come from Kennedy, Dr. Malone and others.
As of January 20, 2022 there were 860,247 COVID Deaths in the US and of that total 645,185 were preventable.
As of January 20, 2022 there were 5,548,704 COVID Deaths in the world and of that total 4,161,528 were preventable.
Fauci is clearly responsible for single handily killing, as of January 21, 2022 (the table is updated daily) 4,161,528 people. Granted others participated in this carnage, but without Fauci, none of this would have been possible so these deaths are 100% on him.
The reason this is true is because he funded and/or directed the “Gain of Function” project and he actively blocked the use of prophylactics for early treatment. That was done so that the mRNA experimental genetic drug could be used. If he had allowed that e.g. Ivermectin, along with a few other prophylactics, be used none of (or most of them) those people would not have died. However the mRNA experimental genetic drug would not have been allowed to be used. So Fauci did this for money for himself and his friends despite the Hippocratic oath that he took.
Byram W. Bridle, PhD, MSc, Associate Professor of Viral Immunology, Department of Pathobiology, University of Guelph, Guelph, ON, Canada, bbridle@uoguelph.ca
Bonnie A. Mallard, PhD, Professor of Immunogenetics, University of Guelph, Guelph, ON, Canada, bmallard@uoguelph.caSubscribe to the Trialsitenews “COVID-19” ChannelNo spam – we promise
Niel A. Karrow, PhD, MSc, Associate Professor, Department of Animal Biosciences, University of Guelph, Guelph, ON, Canada, nkarrow@uoguelph.ca
David J. Speicher, PhD, MSc, Senior Research Associate, Department of Pathobiology, University of Guelph, Guelph, ON, Canada, research@davidspeicher.com
Claudia Chaufan, MD, PhD, Associate Professor of Health Policy and Global Health, York University, Toronto, ON, Canada, claudia.chaufan@protonmail.com
Julian G.B. Northey, PhD, MSc, Adjunct Professor, Ontario Tech. University, Oshawa, ON, Canada, julian.northey@utoronto.ca
Steven Pelech, PhD, Professor, Department of Medicine, University of British Columbia, Vancouver, BC, Canada, spelech@mail.ubc.ca
Christopher A. Shaw, PhD, Professor, Department of Ophthalmology and Visual Sciences, University of British Columbia, Vancouver, BC, Canada, cashawlab@gmail.com
Ondrej Halgas, PhD, MSc, Biomedical Researcher, University of Toronto, Toronto, ON, Canada, ondrej.halgas@mail.utoronto.ca
Deanna McLeod, HBSc, Principal and Lead, Kaleidoscope Strategic, deanna@kstrategic.com
Citation: Bridle BW, Martins I, Mallard BA, Karrow NA, Speicher DJ, Chaufan C, Northey, JGB, Pelech S, Shaw CA, Halgas O, McLeod D. Concerns regarding the efficacy and safety for BNT162b2 mRNA coronavirus disease (COVID-19) vaccine through six months. http://www.CanadianCovidCareAlliance.org (January 10, 2022) 1-10.
Summary of concerns
Efficacy
• Important limitations of the stated efficacy claims were not discussed
• Only the relative risk reductions were stated; absolute risk reduction metrics were not presented
• Integration of adult and adolescent cohorts with differing follow-up periods were presented without explanation
• Large number of discontinued or missing participants comparable to primary end-point event numbers
• Prior SARS-CoV-2 infections screened only in a subset of trial participants, and determined only by an antibody test with severe sensitivity limitations
• Cut-offs of the RT-PCR positivity tests were not reported; no confirmatory functional virology assays were performed
• Absence of systematic testing and unbiased testing framework for the detection of SARS-CoV-2-infected participants
Safety
• Trial participants were healthier than the average population
• Monitoring of adverse events were limited in time and scope
• Number of severe adverse events in the vaccine arm were much higher than the numerical reduction in severe COVID-19 cases between vaccine and placebo arms
• Superficial evaluation of the most clinically relevant end-point – survival; no independent assessment of the causes of death provided
• Cardiovascular adverse vaccine events are now widely recognized, yet no systematic monitoring of cardiovascular health was carried out
• Substantially higher number of solicited and unsolicited adverse events, most of which presented as COVID-19-like symptoms, in the vaccine arm yet study claims efficacy against symptomatic COVID-19
• Increase in cardiac-related deaths in the vaccine arm compared to placebo arm
• Inability to assess long term safety within the trial due to unblinding and participant crossover to the vaccine arm
Other concerns
• Multiple conflicts of interest of a large majority of study authors
• Multiple trial irregularities reported by Thacker et al. (1) published in the British Medical Journal
Article
We present several concerns regarding the recent article by Thomas et al. (2) on the efficacy and safety of the BNT162b2 mRNA coronavirus disease (COVID-19) vaccine, which was published in the New England Journal of Medicine (NEJM) on November 4, 2021. An abbreviated version of this letter was submitted to the NEJM on November 15, 2021 and declined for publication on November 29, 2021 due to limited space. The study assessed the BNT162b2 in individuals that were healthy or had stable chronic medical conditions and concluded that, “through 6 month follow up, despite a gradual decline in vaccine efficacy, BNT162b2 had a favorable safety profile and was highly efficacious at preventing COVID-19.” We present numerous concerns regarding the reported safety and efficacy of this injection.
Efficacy
First, Thomas et al. (2) reported BNT162b2 efficacy as a relative risk reduction of contracting symptomatic reverse-transcriptase-polymerase chain reaction (PCR)-confirmed COVID-19 of 91.3% (77 vs 850 cases) and severe symptomatic PCR-confirmed COVID-19 of 96.7% (1 vs 30 severe cases). Thomas et al. (2) should have reported efficacy as an absolute risk reduction as per the communicating risks and benefits guidelines issued by the United States Food and Drug Administration (FDA) (3), which would have highlighted the modest absolute risk reductions provided by the vaccine in both symptomatic (3.7%) and severe symptomatic (0.7%) PCR-confirmed COVID-19.
Second, this analysis is the only published account of the BNT162b2 phase I – III trial efficacy outcomes among adults ≥16 years of age through six-month follow-up after immunization. In a trial amendment, a cohort of adolescents aged 12 to 15 years was added to the phase III study for which there was a shorter follow-up period. In this analysis, Thomas et al. (2) combined the two cohorts in providing efficacy outcomes after a six month follow up and departed from the initial analysis without providing a reasonable explanation for doing so. Given that vaccine efficacy wanes over time, by combining the older and younger cohorts, Thomas et al. (2) obfuscated the efficacy of the older group at six months. The authors should have provided efficacy outcomes for both groups and explicitly state the two reporting time periods in their conclusion.
Third, when discussing their findings, Thomas et al. (2) did not mention that a larger proportion of participants in the placebo group discontinued the trial compared to the vaccine group; 40% more after the first dose (271 vs 380 participants) and 63% more after the second dose (167 vs 273 participants). Discontinuations consisted mostly of “voluntary withdrawals”, “no longer meeting the eligibility criteria” and “lost to follow-up.” Additionally, there were a high number of participants missing from the CONSORT diagram between 2nd dose and the open-label period with more participants missing in the vaccine arm (1,258 vs 583 missing). These imbalances, which were in the order of the number of primary end-point events (77 and 850, for vaccine and placebo, respectively) call into question the reliability of these findings. Thomas et al. (2) should have disclosed the details related to the nature of these losses and discussed the impact they may have had on overall findings.
Fourth, Thomas et al. (2) used inappropriate tests when assessing current or prior infections due to severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2). The authors screened 10,453 serum samples for COVID-19 infections up to 6 weeks prior to enrollment using the Roche Elecsys® Anti-SARS-CoV-2 antibody test, which tests for only the nucleocapsid protein of SARS-CoV-2 and has high sensitivity 14 days after infection when antibodies tend to peak (4). However, as antibody levels wane over time despite persisting immunity, it is unlikely that this test alone could identify prior immunity to SARS-CoV-2 or distinguish between prior immunity to other coronaviruses, which express similar proteins. Additionally, testing for the SARS-CoV-2 was done with the Cepheid Xpert Xpress SARS-CoV-2 RT-PCR rather than the gold-standard functional virology assay, looking for cytopathic effect in permissive cells. FDA specifications for PCR testing at that time the trial was conducted tended toward cycle thresholds beyond 20-30 cycles (5), which are now widely recognized as being unreliable in detecting an active COVID-19 infection (6-8). Given these limitations, Thomas et al. (2) should have used better screening for natural immunity, used a functional virology assay, and discussed the implications of these testing limitations in their findings.
Fifth, we noted an absence of systematic testing and an objective testing framework for the detection of SARS-CoV-2-infected participants. In this study, it was left to the discretion of the investigator to send a patient presenting with COVID-19-like symptoms for laboratory confirmation of SARS-CoV-2 infection, a task which would be particularly difficult given that reactogenicity events consisted principally of COVID-19-like symptoms (Thomas et al. (2), Figure S1). This lack of systematic testing introduced a concerning level of variability and subjectivity associated with the identification of both symptomatic cases and disease severity (9,10). Thomas et al. (2) should have discussed the implications of this lack of objective and systematic virological assessment on their study findings as well as presented data related to asymptomatic testing that was conducted at “selected sites.” Overall, the emphasis on relative risk reductions, the combining efficacy outcomes from the adult and adolescent cohorts, the large number of people who were excluded from the analysis, and the use of inappropriate tests and lack of objective testing framework call into question the authors’ conclusions regarding vaccine efficacy.
Safety
First, Thomas et al. (2) concluded their article by stating that BNT162b2 showed a “favorable safety profile,” and in their abstract stated that “BNT162b2 continued to be safe and have an acceptable adverse-event profile.” However, Thomas et al. (2) Figure S1 summarized solicited adverse events reported within 7 days of the first dose in the reactogenicity subset, which represented a mere 22% of the randomized population. A considerably higher rate of local and systemic adverse events was reported among vaccine recipients with a marked increase in adverse events with the second dose. The preponderance of systemic effects in both arms were COVID-19-like symptoms and occurred at higher rates than in the vaccine compared to the placebo group, despite the vaccine group having a higher number of identified symptomatic COVID-19 cases (77 vs 850, vaccine vs placebo, respectively). The very need for this trial is predicated on the importance and clinical relevance of eradicating COVID-19 symptoms. How is it then that such consistent increases in COVID-19-like symptoms among vaccine recipients are described as “favorable”?
Second, Thomas et al. (2) provided a descriptive analysis of vaccine safety. To better compare the benefits and the risks of this vaccine, we calculated absolute and relative risk reductions/increases (ARR/ARI and RRR/RRI, respectively) associated with the vaccine for efficacy events seven days after the second dose (i.e., corresponding to full vaccination for those in the vaccine group) and for safety events during the respective data collection period (starting with the first-dose). These calculations were based on the eligible population for each relevant safety and efficacy events without adjusting for surveillance time as that data was not published for safety events. A simple chi-square calculator was used to assess the significance of the difference in event numbers between groups (Table 1) (11).
Table 1. Differences in the number of efficacy and safety events in eligible populations¥ reported in the 6-month update of the BNT162b2 mRNA Covid-19 vaccine
Event
BNT162b2(n)
Placebo(n)
Absolute Difference (p-value)?
Absolute Risk Change* (%)
Relative Risk Change* (%)
Cases Adults and Adolescents 7 days after 2nd dose$
77
850
-773 (p<0.00001)
-3.7
-90.9
Any Unsolicited Treatment-Related Adverse Event Adults#
5,241
1,311
+3,930 (p<0.00001)
+17.9
+299.7
Any Severe Event Adults/
390
289
+101 (p=0.0001)
+0.5
+34.9
Severe Cases in Adults 7 days after 2nd dose&
1
23
-22 (p<0.00001)
-0.1
-95.7
Unsolicited Severe Adverse Events~ AdultsPrevents daily routine activity or requires intervention or worse
262
150
+112 (p<0.00001)
+0.5
+74.6
Serious Adverse Event Adults§Requires hospitalization or results in permanent injury or death
127
116
+11(p=0.5)
+0.05
+9.5
Deaths during placebo-controlled period [additional deaths during open-label period in vaccine recipients or placebo-only]%
15 [+5]
14 [NR]
+1 [+5](p=0.9)
+0.005
+7.1
Deaths due to cardiovascular events^
9
5
+4
¥ For the purpose of this table and in accordance with the terminology used in the study report, adult and adolescent populations are defined as ≥16 years old and 12-15 years old, respectively.
? Significance figures (p-values) estimated using chi-square calculator available at https://www.socscistatistics.com/tests/chisquare. P-values are without the Yates correction. This procedure was applied following the framework used by Classen (11) in his analysis of “All Cause Severe Morbidity” based on data from the initial reports of the vaccine Phase III trials
* Authors estimated vaccine efficacy using total surveillance time as denominator, however, as this value was unavailable for all the events analyzed, our calculations used the common statistical definition, i.e., number of events relative to total number of eligible patients for each event analysis reported29 similar to previous analyses of this nature (11-30);
$ ≥7 Days after dose 2 among participants without evidence of previous infection
# Adverse events reported outside of the reactogenicity subgroup and assessed by the investigator as related to investigational product
/ In calculations combining efficacy and safety events, the number of patients randomized that received any dose of vaccine or placebo was used as the study population in the statistical calculations, following the framework used by Classen (11) in his analysis of “All Cause Severe Morbidity”. Differences in the total (event-incident) population (randomized vs efficacy vs safety) used as denominator are relatively small and are expected to have minimal impact on the relative differences between groups. Without access to individual patient data, these calculations were performed under the assumption that efficacy and safety events were non-overlapping
& ≥7 Days after dose 2; confirmed severe COVID-19 defined as PCR-positivity and “presence of at least one of the following: • Clinical signs at rest indicative of severe systemic illness (RR ≥30 breaths per minute, HR ≥125 beats per minute, SpO2 ≤93% on room air at sea level, or PaO2/FiO2 <300 mm Hg); • Respiratory failure (defined as needing high-flow oxygen, noninvasive ventilation, mechanical ventilation, or ECMO); • Evidence of shock (SBP <90 mm Hg, DBP <60 mm Hg, or requiring vasopressors); • Significant acute renal, hepatic, or neurologic dysfunction;• Admission to an ICU; • Death”
~ Severe (grade ≥3) adverse events were generally defined as those that interfere significantly with participant’s usual function, those that affect daily living or require medical care; grade 4 events were generally defined as those that required emergency room visit or hospitalization
§Serious adverse events were defined as any untoward medical occurrence that, at any dose: a. Results in death; b. Is life-threatening; c. Requires inpatient hospitalization or prolongation of existing hospitalization; d. Results in persistent disability/incapacity.
% Deaths during the open-label period were reported only in vaccine recipients, 3 participants in the BNT162b2 group and 2 in the original placebo group who received BNT162b2 after unblinding
^Those with reported cause of death due to: aortic rupture, arteriosclerosis, cardiac arrest, cardiac failure congestive, cardiorespiratory arrest, hypertensive heart disease, or myocardial infarction
Our findings showed that the increase in unsolicited adverse events in vaccine recipients, which included at least one adverse event up to 1 month post the second dose, was greater (RRI of 299.7% and ARI of 17.9%; p<0.00001) than the reduction in identified symptomatic COVID-19 cases observed in fully-vaccinated individuals for the duration of the trial (RRR of 90.9% and ARR of 3.7%; p<0.00001).
A similar pattern was observed for severe and serious adverse events. The study concluded that “vaccine efficacy against severe disease was 96.7%.” However, our analysis showed that the vaccine was associated with a significant increase in severe adverse events defined as an adverse event that interferes significantly with daily activity or requires medical care (RRI of 74.6% and ARI of 0.5%; p<0.00001) and a numerical increase in serious adverse events, defined as any untoward medical occurrence that was life-threatening, required hospitalization or resulted in persistent disability up to 6 months (RRI of 9.5% and ARI of 0.05%; p=0.5) compared to placebo. These increases were greater than the reduction in severe COVID-19 cases observed in fully-vaccinated individuals for the duration of the trial (RRR of 95.7% and ARR of 0.1%; p=0.00002). When severe COVID-19 events were pooled with severe or serious adverse events to determine the likelihood of experiencing any severe event (11), there was an overall increase in severe events among vaccine recipients compared with placebo (RRI of 34.9% and ARI of 0.5%, p=0.0001). Given these findings, Thomas et al. (2) should have revised their conclusion to state, “the vaccine was associated with a concerning and clinically meaningful increase in severe events relative to placebo.”
Third, Thomas et al. (2) conducted minimal monitoring of adverse events (12). Firstly, the solicited reactogenicity data was collected for only a small portion of trial participants (9,839/44,047 or 22.3%), for a limited 7 days after each dose, and for only a short pre-specified list of systemic and injection site reactions with no monitoring of sub-clinical effects. Secondly, unsolicited adverse events were collected for a mere 1 month and serious adverse events for only 6 months following the second dose. This means that severe vaccine related cardiac, neurological or immunological injuries that took more than a month to diagnose and were not considered serious, would not be reflected in the findings. Thirdly, unblinding and subsequent crossover of those on the placebo arm to the vaccine arm, will certainly attenuate any safety signals coming from this trial as well as preclude insights into long-term safety which were to be monitored for 2 years. Thomas et al. (2) should have commented on the implications their abbreviated monitoring schedule may have on safety underreporting as well as the implications of unblinding on short- and long-term safety outcomes. Given the increase in severe events (RRI of 34.9% and ARI of 0.5%) and cardiovascular deaths associated with the vaccine (n= 9 vs 5, vaccine vs placebo, respectively), The authors should have more closely monitored safety and provided a detailed discussion of the severe and serious adverse events along with a discussion of their potential long-term implications.
Fourth, given the inclusion of adolescents and “healthy participants who had stable chronic medical conditions” in the study population, we noted very little discussion of death, the most clinically relevant end-point of this trial. Thomas et al. (2) Table S3 showed a slightly higher number of deaths in the vaccine group (n=15 vs n=14 in the placebo group during the blinded period). However, the manuscript text (Thomas et al. (2), page 7) stated that five additional deaths occurred in vaccine recipients after unblinding (two of which were initially allocated to the placebo group) for a total of 20 deaths in vaccine recipients. Thomas et al. (2) Table S4 also showed that although only 3 study deaths were attributed to COVID-19 or COVID-19 pneumonia (n=1 vs n=2, vaccine vs placebo, respectively) a total of 14 deaths were cardiovascular in nature (aortic rupture, arteriosclerosis, cardiac arrest, cardiac failure congestive, cardiorespiratory arrest, hypertensive heart disease) with the almost twice as many occurring in the vaccine arm (n=9 vs n=5, vaccine vs placebo, respectively). There is currently an abundance of real-world evidence to support an association between cardiovascular adverse events and the vaccines (13-17). Thomas et al. (2) reported that “none of these deaths were considered to be related to BNT162b2 by the investigators” without describing the objective framework of testing that allowed them to arrive at that conclusion or whether their findings were independently evaluated. Given the seriousness of these adverse events in an otherwise healthy population, Thomas et al. (2) should have provided a detailed description of how they arrived at their conclusion, these evaluations should have undergone independent assessment, and all ongoing study protocols investigating BNT162b2 should be immediately amended to include systematic short- and long-term clinical and sub-clinical monitoring of cardiovascular health. Overall, the increased rates of COVID-like symptoms, unsolicited adverse events as well as severe and serious adverse events in the vaccine compared to the placebo arm, as well as the net increase in deaths in vaccine recipients compared with those who were unvaccinated present serious concerns regarding the safety of these biological agents.
Conflicts of Interest
The disconnect between author conclusions, our analysis of the data, and the NEJM rejection of our letter to the editor led us to examine author disclosures for potential conflicts of interest (COI) (Table 2). Our analysis revealed multiple direct conflicts of interest. The article was supported by BioNTech and Pfizer, the corresponding author, Judith Absolon, and the senior author, Kathrin Jansen were employees of Pfizer and owned company stock, and the first author Stephen Thomas was a consultant to Pfizer. Of the 32 authors, 21 (66%) were employees of Pfizer or BioNtech and 26 (81%) had Pfizer/BioNtech-related conflict of interests. We also noted that one of NEJM’s senior editors is also a co-principal investigator of the related Moderna-Vaccine COVE-trial (18,19).
Table 2. Conflicts of interest related to Pfizer/BioNTech
Title
Author
Corresponding author
Judith Absalon: Pfizer employment and stock holder
First author
Stephen Thomas: Pfizer consultancy
Last author
Kathrin Jansen: Pfizer employment and stock holder
Other 29 authors (66% employees, 81% had some COI)
Pfizer/ BioNTech employment and stockholder, n=15; Pfizer/ BioNTech employment (without stock) n=4; Pfizer grant/contract n=3; Pfizer clinical trial n=1; Other company consultancy n=1; No COI n=5
Conclusion
Our critique of the Thomas et al. (2) publication revealed multiple concerns regarding author claims of BNT162b2 safety and efficacy as well as a high number of direct conflicts of interest in the publication authors. These, coupled with multiple reports indicating that vaccine efficacy wanes within months of administration (20-23), reduced effectiveness of BNT162b2 with respect to emerging variants (24-26), record rates of serious adverse events (122,833) and deaths (17,128) reported in the US passive Vaccine Adverse Event Reporting System, VAERS by October 16, 2021, and problems with data integrity in the conduct of this trial reported recently by Thacker (1) in the British Medical Journal, raise further concerns regarding both the efficacy and safety of this agent. We did not find sufficient evidence to support use of these agents in the healthy adults studied or in specific unstudied demographics that are being mandated to comply with vaccination including the naturally immune, the frail elderly, those with multiple co-morbidities, the immunocompromised, and pregnant women. It also calls into question use in adolescents and children given that companion trials conducted in those populations suffered from similar design flaws, including underpowered in participant numbers and that recommendations for use were based on minimal safety follow up (27,28).
Conflicts of Interest
Byram W. Bridle received funding from the Ontario Government (COVID-19 Rapid Research Fund, Ministry of Colleges and Universities) and Government of Canada (Pandemic Response Challenge Program, National Research Council of Canada) to conduct pre-clinical research with COVID-19 vaccines
Ilidio Martins, none to disclose
Claudia Chaufan, none to disclose
Julian Northey, none to disclose
Niel A. Karrow, none to disclose
Steven Pelech is the majority shareholder and president and Chief Scientific Officer of Kinexus Bioinformatics Corporation, which has been developing serological tests for detection of antibodies against SARS-CoV-2 proteins and testing of drugs to inhibit SARS-CoV-2 replication
Bonnie Mallard, none to disclose
Christopher A. Shaw has been an expert witness in Vaccine Court twice
David Speicher, none to disclose
Ondrej Halgas, none to disclose
Deanna McLeod, none to disclose
References
1. Thacker PD. COVID-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial. BMJ 2021;375:n2635.
2. Thomas SJ, Moreira ED, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine through 6 months. N Engl J Med 2021;385:1761-73.
3. Fischhoff B. Communicating risks and benefits: An evidence based user’s guide. Silver Spring, MA, USA: Food and Drug Administration (FDA), US Department of Health and Human Services. Government Printing Office; 2012.
5. Cepheid. Xpert® Xpress SARS-CoV-2 – Instructions for use. For use under an Emergency Use Authorization (EUA) only. U. S. Food and Drug Administration, 2021. (Accessed June 29, 2021, at https://www.fda.gov/media/136314/download.)
6. Mina MJ, Peto TE, García-Fiñana M, Semple MG, Buchan IE. Clarifying the evidence on SARS-CoV-2 antigen rapid tests in public health responses to COVID-19. The Lancet 2021;397:1425-7.
7. Al Bayat S, Mundodan J, Hasnain S, et al. Can the cycle threshold (Ct) value of RT-PCR test for SARS CoV2 predict infectivity among close contacts? Journal of Infection and Public Health 2021;14:1201-5.
11. Classen B. US COVID-19 vaccines proven to cause more harm than good based on pivotal clinical trial data analyzed using the proper scientific endpoint,“All cause severe morbidity”. Trends Int Med 2021;1:1-6.
13. Rose J. A Report on the US Vaccine Adverse Events Reporting System (VAERS) of the COVID-19 messenger ribonucleic acid (mRNA) biologicals. Sci, Pub Health Pol, & Law 2021;2:59-80.
14. Kaur RJ, Dutta S, Charan J, et al. Cardiovascular adverse events reported from COVID-19 vaccines: A study based on WHO database. Int J Gen Med 2021;14:3909.
15. Aye YN, Mai AS, Zhang A, et al. Acute myocardial infarction and myocarditis following COVID-19 vaccination. QJM: monthly journal of the Association of Physicians 2021.
16. Diaz GA, Parsons GT, Gering SK, Meier AR, Hutchinson IV, Robicsek A. Myocarditis and pericarditis after vaccination for COVID-19. JAMA 2021;326:1210-2.
17. Barda N, Dagan N, Ben-Shlomo Y, et al. Safety of the BNT162b2 mRNA COVID-19 vaccine in a nationwide setting. N Engl J Med 2021;385:1078-90.
18. Baden LR, El Sahly HM, Essink B, et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med 2021;384:403-16.
19. Keil U. Re: COVID-19: How independent were the US and British vaccine advisory committees? BMJ 2021;373:n1283. 2021. (Accessed Dec 6, 2021, at Re: COVID-19: How independent were the US and British vaccine advisory committees?)
20. Goldberg Y, Mandel M, Bar-On YM, et al. Waning immunity after the BNT162b2 vaccine in Israel. N Engl J Med 2021.
21. Puranik A, Lenehan PJ, O’Horo JC, et al. Durability analysis of the highly effective BNT162b2 vaccine against COVID-19. medRxiv 2021.
22. McDade TW, Demonbreun AR, Sancilio A, Mustanski B, D’Aquila RT, McNally EM. Durability of antibody response to vaccination and surrogate neutralization of emerging variants based on SARS-CoV-2 exposure history. Sci Rep 2021;11:1-6.
23. Andrews N, Tessier E, Stowe J, et al. Vaccine effectiveness and duration of protection of Comirnaty, Vaxzevria and Spikevax against mild and severe COVID-19 in the UK. medRxiv 2021.
24. Collie S, Champion J, Moultrie H, Bekker L-G, Gray G. Effectiveness of BNT162b2 vaccine against Omicron variant in South Africa. N Engl J Med 2021.
25. Lefèvre B, Tondeur L, Madec Y, et al. Beta SARS-CoV-2 variant and BNT162b2 vaccine effectiveness in long-term care facilities in France. The Lancet Healthy Longevity 2021;2:e685-e7.
26. Hansen CH, Schelde AB, Moustsen-Helm IR, et al. Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study. medRxiv 2021:2021.12.20.21267966.
27. Frenck RW, Jr., Klein NP, Kitchin N, et al. Safety, immunogenicity, and efficacy of the BNT162b2 COVID-19 vaccine in adolescents. N Engl J Med 2021;385:239-50.
28. Walter EB, Talaat KR, Sabharwal C, et al. Evaluation of the BNT162b2 COVID-19 vaccine in children 5 to 11 years of age. N Engl J Med 2021.
I have created this site to help people have fun in the kitchen. I write about enjoying life both in and out of my kitchen. Life is short! Make the most of it and enjoy!
This is a library of News Events not reported by the Main Stream Media documenting & connecting the dots on How the Obama Marxist Liberal agenda is destroying America