By Habibi Bros. Published originally on Rumble on August 17, 2022
Siraj and Jay discuss the CDC admitting to f*cking up the COVID-19 pandemic response, Liz Cheney gets ousted from Congress, developments in the FBI raid of Trump’s home at Mar-A-Lago, and the one-year anniversary after the catastrophic Afghanistan withdrawal. It’s everything that makes you want to drink on Habibi Power Hour.
The Biden Administration declared a public health emergency over monkeypox. This is not an airborne virus, and it is fairly difficult to catch as skin-to-skin contact is the primary method of transmission. The woke media does not want this fact released, but the Centers for Disease Control and Prevention (CDC) has found that 99% of all cases were found in men, and 94% have had male sexual encounters.
Additionally, nearly 20% of gay men who fell ill admitted to having 10 or more partners in the three weeks before symptoms began. About 40% of those who fell ill reported having two to four partners, while 14% reported having five to nine partners. Around 38% admitted to participating in group sex.
This is more of a sexually transmitted disease and should be presented to the public as such. CDC guidance:
“Public health efforts should prioritize gay, bisexual, and other men who have sex with men, who are currently disproportionately affected, for prevention and testing, address equity, and minimize stigma, while maintaining vigilance for transmission in other populations.”
There is no need to stigmatize people for their sexual preferences or repeat problematic misinformation that spread during the 80s during the AIDS epidemic. However, there is no need to scare the general public into thinking that monkeypox is easily transmissible. If they care about health (they don’t), then they should be honest about the virus and educate the demographic mainly at risk.
Geert Vanden Bossche, DVM, PhD General Manager at Voice for Science and Solidarity | The biggest challenge in vaccinology: Countering immune evasion originally published on TS News on Aug. 5, 2022
MIS-C is a disease that may occur in school-age children two to six weeks after infection with SARS-CoV-2 (SC-2) virus. MIS-C is a post-infectious inflammatory condition which typically occurs after asymptomatic/mild SC-2 infection. Some children may need hospitalization because of inflammatory reactions in different organs. While the syndrome can be serious, the absolute risk for MIS-C is very low (about 6.5 per 100 000 person-years) and known to be increased in boys aged 5-11 years with foreign-born parents, asthma, obesity, and life-limiting condition (https://www.thelancet.com/action/showPdf?pii=S2666-7762%2822%2900137-5). MIS-C mostly resolves within a few days after timely and adequate (immunosuppressive) treatment. As the pandemic evolves and more infectious Omicron (sub)variants are now dominating the scene, MIS-C is occurring less frequently and with diminished severity of disease (https://jamanetwork.com/journals/jama/fullarticle/2792718). This evolution cannot be entirely explained by C-19 vaccination of young children as vaccine coverage rates in this age group are still very low (15% and 3% as recently reported in studies from Israel and the US, respectively; https://jamanetwork.com/journals/jama/fullarticle/2792718; https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciac471/6605071). It is therefore tempting to speculate that enhanced viral infectiousness and transmission significantly contribute to dampening the incidence rate and severity of MIS-C in young children. This suspicion is supported by a previous study in which the authors speculated that some of the risk factors they identified for MIS-C could be associated with enhanced disease transmission (e.g., in children with foreign-born parents or explaining the shift in age from 12-15 years down to 5-11 years amongst children with MIS-C throughout the pandemic (https://www.thelancet.com/action/showPdf?pii=S2666-7762%2822%2900137-5).
To better understand the origin of the disease, and why children in particular are susceptible to contracting MIS-C, it is important to understand how the child’s innate immune system is educated and trained to combat infections with glycosylated viruses causing acute self-limiting viral infection (ASLVI; e.g., SC-2) or acute self-limiting viral disease (ASLVD).
The child’s innate immune system first learns to discern relevant pathogen-derived molecular patterns and discriminate them from self-derived motifs. Once the child’s natural killer (NK) cells have been ‘educated[1]’ (pre-primed) to adequately sense and distinguish pathogen-derived self-mimicking peptides (PSMPs) from self-derived self-mimicking peptides, presentation thereof in high density patterns may trigger epigenetic changes that imprint these NK cells with memory (so-called ‘training’ of NK cells).
In young children who have cleared their maternal antibodies (around the age of 6 months), abundantly produced innate (sometimes called ‘natural’) antibodies (Abs) play a critical role in initiating active use of their own immune system. In these children, innate Abs are tasked with recognizing and binding free-circulating self-derived glycan motifs (e.g., decorating foreign-derived [including pathogen-derived] or self-derived proteins) to potentiate[2] the presentation of repetitive patterns of foreign- or self-derived self-mimicking peptides on the surface of autologous somatic cells or antigen (Ag-)presenting cells (APCs). Glycosylation of self-proteins is an important mechanism for inducing T cell-mediated peripheral tolerance[3] and, not surprisingly, mimicked by several pathogens (e.g., glycosylated viruses) as a strategy to subvert the host immune system. As they decorate themselves with self-mimicking patterns of self-glycans, glycosylated viruses (e.g., corona virus [CoV], influenza virus, respiratory syncytial virus [RSV], measles, mumps, rubella, varicella virus,…) can be recognized and captured by innate Abs and thereby contribute to educating the child’s innate immune effector cells (i.e., NK cells).
As the child grows up, the functional capacity of their innate Abs gradually declines so that their immune system can progressively replace the ‘self’-sensing innate Ab capacity by a pool of pre-primed NK cells that can recognize pathogen-derived self-mimicking (i.e., ‘altered self’) motifs on virus-infected or otherwise pathologically altered host cells such as to kill those cells. For as long as a child possesses an abundant functional capacity of innate Abs, glycosylated pathogens and self-ligands will be complexed by innate Abs to educate NK cells on how to distinguish ‘self’ from ‘non-self’. This is how the innate immune system of the young child is thought to ‘adapt’ to the early-life extra-maternal environment where it must learn to rapidly sense peptide motifs that differ from self-peptides. This would enable NK cells to target and kill autologous host cells that are decorated with such ‘altered self’ peptides (e.g., infected, or otherwise pathologically altered host cells).
Once NK cells are educated, the NK cell training process dictates their functional re-programming (https://www.frontiersin.org/articles/10.3389/fimmu.2018.01869/full). Training is thought to result from epigenetic alterations that are triggered by changes in the SC-2 infectious landscape and generate ‘adaptive’ or ‘memory-like’ NK cells. Adequate training of its first line of immune defense enables the child to mount protective natural immunity against SC-2 (and other glycosylated viruses/ pathogenic agents sharing the same PSMPs[4]) upon future exposure. This can already explain why prophylactic childhood vaccinations using live attenuated virus are very efficient at inducing natural immunity against measles, mumps, rubella, varicella and generating herd immunity−it’s only when they become infected with an antigenically ‘shifted’ (i.e., very different) variant that individuals who acquired natural immunity can still contract disease due to ADEI.
However, depending on viral infectious pressure, it is perfectly possible, even for a young and healthy child, to become susceptible to productive infection upon exposure to glycosylated, ASLVI-enabling viruses that do not normally cause symptomatic infection in young children.
When young and healthy children become infected during an outbreak of a virus with a relatively low reproduction number (R0; e.g., infection with common cold coronavirus [CoV] or seasonal Flu; R0 < 2.5), they almost always develop asymptomatic or very mild infection. However, dominant circulation of more infectious CoV or Influenza virus variants can occasionally provoke cases of severe disease in children. It is reasonable to postulate that enhanced viral infectiousness raises the chance for a person to become re-infected shortly after a previous course of asymptomatic infection. This will increase the likelihood that immature, short-lived Ag-specific Abs[5] of relatively low affinity, which typically develop after asymptomatic/ mild infection, will still be present when that person becomes re-exposed to the virus. Because of their Ag-specificity, these Abs may outcompete the child’s innate polyspecific IgM Abs, which have an even lower affinity for the protein Ag that is responsible for initiation of infection (i.e., spike [S] protein in the case of CoV). Depending on their titer, these non-neutralizing, Ag-specific Abs can therefore prevent or at least diminish binding of innate Abs to the virus. Although these short-lived Abs cannot neutralize the virus, they can bind to it and enhance its infectiousness.
This is particularly problematic in young children as insufficient training of their NK cells prevents effective immune targeting of SC-2-infected cells expressing virus-derived self-mimicking peptides on their surface. NK cells that are largely ‘pathogen-inexperienced’ together with enhanced SC-2 infectiousness would entail enhanced susceptibility of young children to SC-2 infection (i.e., so called ‘Ab-dependent enhancement of viral infectiousness’; ADEI). Hence, re-infection shortly after previous asymptomatic exposure will likely allow the virus to break through the cell-based innate immune system of young children and could potentially cause (severe) disease (https://pubmed.ncbi.nlm.nih.gov/33391280/). However, as these post-infectious Abs wane rapidly (they are no longer detectable at about 8 weeks), only a limited number of children will become re-exposed to the circulating virus shortly after their previous productive exposure. This already explains why most cases of MIS-C occur between 2 and 6 weeks (on average 4 weeks) after the previous asymptomatic/ mild infection, presumably depending on the titer of the infection-enhancing Abs at the timepoint of re-exposure. It is therefore not surprising to also observe high variability in the severity of MIS-C disease.
More infectious SC-2 variants may enable stronger stimulation of NK cells and thereby readily prime NK cell effector responses in young children; alternatively,more infectious SC-2 variants could increase the likelihood for viral re-exposure to occur in the presence of a relatively higher titer of infection-enhancing anti-S Abs. Both phenomena are likely to reduce the risk of MIS-C in young children.
After many years of NK cell vaccine research (which I was unable to publish for intellectual property reasons), I determined that the recruitment on MHC class I molecules of PSMPs into ‘non-self’ high-density arrays (situated outside of the MHC class I peptide-binding groove!) is what allows for activation and epigenetic imprinting (i.e., training) of cytotoxic NK cells that are capable of killing host cells that present such PSMPs on their surface (for example as a result of viral infection). I postulate that strong stimulation by enhanced viral infectiousness could even obviate the need for cumulative triggering of NK cells (so-called ‘training’) in order for NK effector cells to become imprinted with memory. NK cells that have acquired a memory-like phenotype could readily eliminate host cells that are infected with relevant glycosylated pathogens. Enhanced viral infectiousness in the young child could allow productive SC-2 infection even in the presence of innate Abs and thereby enable ‘power training’ of pre-primed NK cells. Even though symptoms could still be mild, productive infection would have the capacity to substitute a single ‘power training’ event for regular, incremental training of functional NK cell responsiveness to pathogen-derived ligands. As full-fledged NK cell ‘priming’ towards PSMPs would therefore improve with enhanced viral infectiousness, C-19 unvaccinated children (and even some adolescents) who recently contracted mild disease would be equipped with innate immune memory while no longer developing infection-enhancing anti-S Abs (as shown in fig. 1). Alternatively, enhanced viral infectiousness leads to higher viral infection rates and thereby shortens the average time window for a person to become re-exposed after a previous asymptomatic SC-2 infection. A shortened window for re-exposure makes it more likely that the latter occurs in the presence of a relatively high titer of infection-enhancing Abs. It is not unreasonable to assume that the mechanism of naturally induced infection-enhancing Abs is similar to the one previous described for vaccine-induced anti-S Abs−a high enough concentration of these Abs would allow a subset of these Abs to bind to SC-2 virions tethered to dendritic cells and thereby exert a disease-mitigating effect (https://www.voiceforscienceandsolidarity.org/scientific-blog/predictions-gvb-on-evolution-c-19-pandemic + fig. 2).
Based on the rationale explained above, one could easily understand how the prolonged C-19 pandemic and the enhanced frequency of repetitive waves of more infectious variants (e.g., Omicron) is likely to have a ‘power training’ effect on relevant NK cells of young C-19 unvaccinated children developing mild primary infection (i.e., overlapping with abundant functional capacity of innate Abs) or to provide a strong disease-mitigating adaptive immune response in those who recently contracted asymptomatic SC-2 infection. The latter would be protected from severe and even moderate disease by virtue of infection-enhancing Abs and cytotoxic CD8+ T cells, respectively (as illustrated in fig. 2). A further increase in viral infectiousness would not make young, previously asymptomatically infected children more susceptible to disease but rather increase their likelihood to develop productive SC-2 infection and generate effector memory NK cells or further expand those (as shown by the arrows in green in fig. 1). With this understanding, it is not surprising that the advent of Omicron (sub)variants has led to a rapidly regressing incidence rate and severity of MIS-C (https://jamanetwork.com/journals/jama/fullarticle/2792718).
How does mass vaccination affect the child’s susceptibility to SC-2 infection?
As the mass vaccination program during this pandemic has led to the dominant circulation of more infectious SC-2 variants, it is not surprising to find that a few, young (C-19 unvaccinated) children contracted MIS-C and even needed hospitalization—this was an extremely rare event at the beginning of the pandemic. However, the mass vaccination program has provided immune escape variants characterized by a higher level of intrinsic viral infectiousness (e.g., of the delta variant) with a competitive advantage. The ensuing higher infection rate in the population (and in households!) therefore came with an additional likelihood for young children to become re-infected shortly after their previous asymptomatic infection. As previously described, the incidence rate of MIS-C is now waning as a result of enhanced innate immune training and mitigation of (severe) disease by more and more infectious SC-2 variants that have now become dominant.
Vaccinating children against SC-2 is a colossal scientific blunder with potentially disastrous health consequences
More importantly, the currently circulating Omicron (sub)variants are already endowed with higher intrinsic virulence that–for now–is still kept in check by the virulence-inhibiting activity of infection-enhancing anti-S Abs (as reviewed in: https://www.voiceforscienceandsolidarity.org/scientific-blog/predictions-gvb-on-evolution-c-19-pandemic). We have already witnessed how more infectious variants developed resistance to potentially infection-neutralizing Abs induced by C-19 vaccines and there is little doubt that more virulent SC-2 lineages will manage a similar ‘trick’ to develop resistance to potentially virulence-‘neutralizing’ Abs (especially since repeated exposure to more infectious circulating Omicron (sub)variants will recall these vaccinal S-specific Abs and thereby ensure sustained immune pressure). When this happens, vaccinated infants and toddlers will be left with an adaptive immune system that does no longer protect them from severe C-19 disease and with NK cells that have not been trained due to prolonged suspension of their education (https://www.trialsitenews.com/a/intra-pandemic-vaccination-of-toddlers-with-non-replicating-antibody-based-vaccines-targeted-at-aslvi1-or-aslvd2-enabling-glycosylated-viruses-pr-66e8b959). Prolonged sidelining of the child’s innate Abs is thought to hamper the functional capability of cytotoxic NK effector cells to sense and target virus-derived, molecular self-mimicking peptides that are expressed on virus-infected host cells. As already reported, lack of innate immune education could dramatically impede the child’s capacity to generate natural immunity to SC-2 in particular as well as other ASLVI- or ASLVD-enabling glycosylated viruses in general (https://www.trialsitenews.com/a/epidemiologic-ramifications-and-global-health-consequences-of-the-c-19-mass-vaccination-experiment-a212bb47).
On the other hand, diminished complexation of foreign glycosylated ligands by innate Abs could render NK cells that lack self-MHC-I inhibitory receptors hyporesponsive to stimulatory receptor activation as a result of their chronic low-level stimulation by self-derived peptides. Because of the resulting diminished threshold of NK cell activation in the periphery, young C-19 vaccinated children would be prone to developing immunopathologies. However, in the likely event that resistance to potentially virulence-‘neutralizing’ Abs develops, it can be expected that−given the high SC-2 infection rate− C-19 vaccinated infants and toddlers will primarily succumb to Ab-dependent enhancement of severe C-19 disease rather than to severe disease from any other circulating ASLVI or ASLVD or from immunopathology.
Conclusion
Increased SARS-CoV-2 exposure results from dominant expansion of more infectious SC-2 variants, a phenomenon undeniably caused by the C-19 mass vaccination program. As suggested by the results from earlier studies, increased exposure to SC-2 together with a number of predisposing factors renders very few young children susceptible to developing MIS-C following a recent asymptomatic infection (https://www.thelancet.com/action/showPdf?pii=S2666-7762%2822%2900137-5). There is no doubt that vaccinating children against SC-2 is a colossal blunder and merely places the child at high risk of severe health damage. MIS-C has not only a low incidence (which is further declining) but can also be successfully treated using conventional drug therapy. This contrasts with the protective effect of C-19 vaccination against MIS-C, which is temporary and leaves the young child at high risk of contracting Ab-dependent enhancement of severe disease upon future exposure to new SC-2 variants (which will dominantly emerge as a result of the current population-level immune pressure on viral virulence). It is critical to understand that the high viral infection rate in highly C-19 vaccinated populations due to mass vaccination, rather than a lack of C-19 vaccination, is responsible for this phenomenon. There is therefore no single scientific rationale for vaccinating children against SC-2−exactly the contrary is true: C-19 vaccination of young children is highly likely to not only provoke a soaring incidence of severe disease and mortality due to immunopathology and other microbial diseases but ultimately also due to SC-2. Public health authorities are creating the illusion for parents that C-19 vaccines will protect their children, instead of educating them how to recognize early signs and symptoms of MIS-C in order to seek highly effective treatment for their child in due time. In addition, they seem to ignore that preserving natural immunity in young children is critical as it is the key pillar of herd immunity to ASLVIs, including SC-2.
Figures
Fig. 1: Upon exposure to more infectious SC-2 variants, young children may develop MIS-C as a result of re-exposure shortly after previous asymptomatic infection. However, as their infectiousness increases, new SC-2 variants may break through the child’s innate Ab-mediated protection and thereby cause mild infection that imprints its NK cells with memory and therefore dramatically boosts the child’s first line of immune defense. Alternatively, more infectious variants enable re-exposure in the presence of higher titers of short-lived infection-enhancing anti-S Abs. In the latter case, young children are protected from severe disease presumably because a subset of anti-S Abs can bind to SC-2 virions tethered to dendritic cells (see fig. 2), thereby inhibiting severe/systemic disease whereas sustained activation of CTLs (as a result of the infection-enhancing capacity of these Abs upon their binding to free virions) further mitigates C-19 disease. Both scenarios may be responsible for the observed reduction in the incidence rate and severity of MIS-C as the pandemic continues to evolve (indicated by “–“ and arrows in blue). Since the pandemic has now evolved highly infectious SC-2 variants (i.e., the new Omicron [sub]variants), viral exposure of young children is more and more likely to readily cause mild infection resulting in NK cell ‘power training’ and further expansion of effector memory NK cells upon a further increase in viral infection rates (indicated by “+” and arrows in green). This may ultimately prevent young children from developing MIS-C all together.
Fig. 2(from https://www.trialsitenews.com/a/epidemiologic-ramifications-and-global-health-consequences-of-the-c-19-mass-vaccination-experiment-a212bb47): Acute, self-limiting viral infections that don’t lead to systemic/severe disease (and possibly death) are terminated by M(ajor) H(istocompatibility) C(omplex)-unrestricted, cytotoxic CD8+ T cells that have no memory and the activation of which is triggered by a universal, pathogen-nonspecific Tc epitope comprised within the spike (S) protein. Unless an infected person progresses to developing severe disease, this is what allows a fairly rapid recovery from disease after primary productive infection (and certainly before fully functional virus-neutralizing Abs peak) [according to 2a-2b-2c-2d pathway]. However, rather than stimulating de novo generation of new neutralizing Abs towards variants that escaped the neutralizing activity of vaccine-induced Abs, exposure of vaccinees to these immune escape variants will rapidly boost their declining titers of non-neutralizing, infection-enhancing Abs (those are directed against an antigenic site that is conserved within the N-STD of all SC-2 variants and has therefore a license to commit ‘antigenic sin’ once it has primed the host’s immune system).
In vaccinees with poor experience in fighting productive infection (and hence, poor training of their innate immune defense according to pathway 1a-1b-1c) prior to C-19 vaccination, infection-enhancing Abs[6] that are responsible for preventing severe disease by binding to DC-tethered virus (according to 3a-3b-3c-3d pathway) can synergize with strongly activated cytotoxic CD8+ Tc-mediated killing (3c’) to even prevent C-19 disease all together and hence, render vaccinees asymptomatic despite their high susceptibility to re-infection (B + C ? D). As prevention of disease is not due to prevention of productive infection but to accelerated abrogation of infection, these vaccinees will continue to shed and transmit SC-2 upon re-infection. Whereas innate immune effector cells are MHC-unrestricted and polyspecific (i.e., NK cells) and, therefore, don’t drive immune escape, the infection-enhancing-Abs are Ag-specific (i.e., S-specific) and – if produced at high enough titers and with high enough affinity by a large part of the population – will promote natural selection of immune escape variants that can resist the virulence-inhibiting capacity of these Abs. This is because vaccinees cannot prevent productive viral infection; consequently, the immune pressure they exert on viral virulence is suboptimal in that it cannot prevent the expansion in prevalence of immune escape SC-2 variants that have the capacity to overcome this immune pressure. Resistance of viral variants to the virulence-inhibiting activity of infection-enhancing Abs will inevitably cause Ab-dependent enhancement of severe disease (ADESD).
1. Education of NK cells that lack self-MHC-I inhibitory receptors but are endowed with germline-encoded NK cell activation receptors dictates their functional capability to recognize self- or pathogen-derived self-mimicking ligands and mediate innate effector functions; https://www.frontiersin.org/articles/10.3389/fimmu.2018.01869/full
2. Besides their neutralizing activity, natural/innate Abs can, indeed, serve as immune potentiators (‘natural adjuvants’) to upregulate the presentation of antigens on cell surface-expressed MHC class I molecules https://pubmed.ncbi.nlm.nih.gov/14502281/)
4. Enveloped glycosylated viruses are critical to educate the child’s innate immune system in ways that allow recognition and elimination of somatic cells expressing PSMPs (as a result of viral infection or other pathologic alteration) which may otherwise induce tolerance (e.g., cancer cells) or provoke autoreactive or immune inflammatory responses (i.e., causing autoimmune or hyperinflammatory disease, respectively).
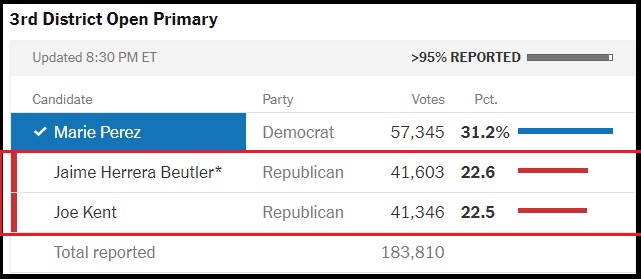
Jamie Herrera Beutler, who voted to impeach President Trump and is one of the MAGA targets for 2022, now has 41,603 votes. Trump-endorsed Joe Kent has moved from a several thousand vote deficit, into the latest result of 41,346 votes. The difference is now down to 257 votes.
Washington State has that jungle primary voting system where the top two candidate’s face-off in the general election. According to Kent on Twitter, there are 30,000 ballots left to be counted. Prayers up!! Joe Kent might just pull off this victory.
If the next batch of 30,000 ballots, carries the same ratio as today’s batch of 22,000 ballots, Joe Kent will take the lead.
I’m only 1% behind RINO Beutler despite millions spent against me & the establishment supporting 2 spoiler candidates to split the MAGA vote.
Posted originally on the conservative tree house on August 5, 2022 | Sundance
President Trump travels to Waukesha, Wisconsin tonight for a MAGA rally to support Tim Michels for Governor and all of the down ballot republican candidates. With the overwhelming MAGA victories in Michigan, Arizona and Missouri this week, there is a lot for President Trump to celebrate.
The scheduled start time is 7:00pm CT / 8:00pm ET. Rumble Livestream Links Below:
Georgia law states that life begins at conception. Aside from cases of rape and incest, or if the mother’s life is in danger, abortions are prohibited in the state. The Georgia Department of Revenue (DOR) has stated that the Dobbs v. Jackson Women’s Health Organization ruling sees the unborn as “natural persons.”
Therefore, under that logic, the unborn child has Constitutional rights. Georgia’s tax department will now allow taxpayers to claim unborn children as dependents. “Department will recognize any unborn child with a detectable human heartbeat … as eligible for the Georgia individual tax dependent exemption,” the DOR stated. Tax exemptions may reach $3,000 per unborn child. A heartbeat may be detected as early as six weeks into pregnancy via ultrasound.
Even some liberal voices are praising this new law as it will help low-income families who need the extra money. Other states strongly opposed to the practice of abortion may follow suit. Let’s just hope the government doesn’t find a way to tax unborn persons.
NorthShore University HealthSystem in Chicago was sued by a nonprofit religious organization called Liberty Counsel. The group claims that NorthShore violated workers’ religious autonomy by dismissing religious exemptions and forcing all workers to receive the COVID-19 vaccine. NorthShore was in the wrong and decided to settle for $10,337,500.
Other groups will follow suit. They may have granted the pharmaceutical companies immunity, but there was a grey area for employers. Countless people lost their jobs due to the vaccine mandate, which likely was a violation of the Constitution.
Lawsuits may begin with large corporations, but if the Republicans regain control, health agencies and government officials may be investigated as well. This lawsuit is a major win for medical autonomy as companies will be less likely to comply with government mandates as they now know they could risk legal retaliation.
I have created this site to help people have fun in the kitchen. I write about enjoying life both in and out of my kitchen. Life is short! Make the most of it and enjoy!
This is a library of News Events not reported by the Main Stream Media documenting & connecting the dots on How the Obama Marxist Liberal agenda is destroying America