Posted originally on the conservative tree house on January 16, 2022 | Sundance | 181 Comments
Quite remarkably this ABC report on empty shelves is not far away from outlining the truth. They are still obfuscating some of the predictable reasons, and they completely ignore the vaccination mandate aspect that is going to worsen the issue, but they are nibbling the edges, nonetheless.
The backward-looking comparative statistics they cite, “15% shortage for food and beverages” overall, are nonsense. The severity of unavailable products is much higher than that. You will note from your own store visits the most unavailable products are the manufactured food and heavily processed products.
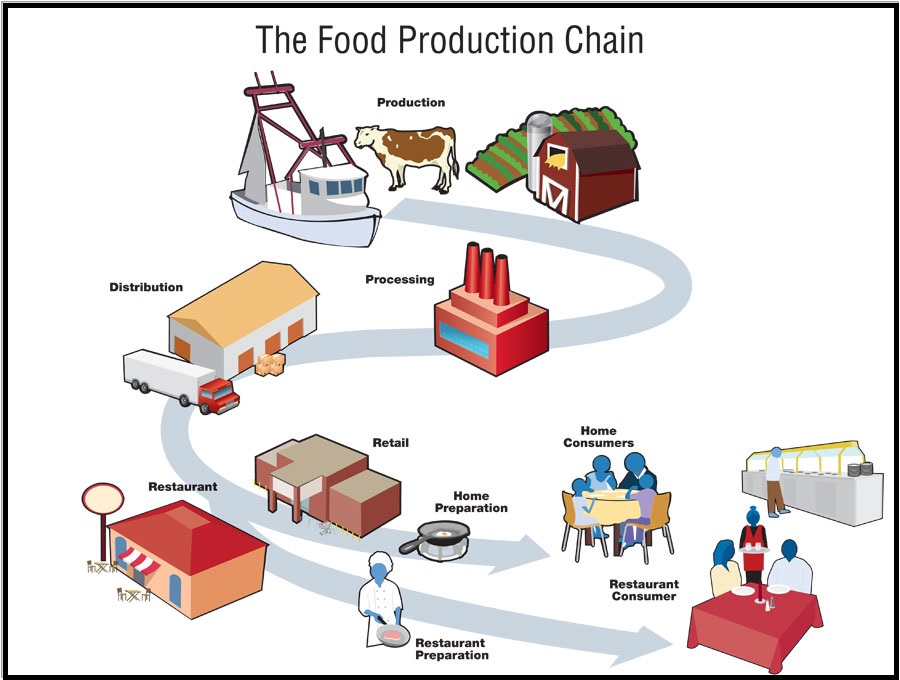
The raw material shortage inside the retail manufacturing supply chain path, combined with the increased demand on those manufactured sectors, is the direct cause of the manufactured food shortage. {Go Deep} [Example: a high demand for citric acid means complex foods that use citrus flavorings (ie. sports drinks) are in short supply. Chase that backward, and you see shortages in citrus & higher citrus costs, etc.]
Each seemingly small issue creates another small issue, which creates another small issue, which ultimately pokes holes in the supply. Poke enough holes in enough small categories from manufactured condiments to manufactured drinks, to manufactured cereals, pasta, grains, soups, pet foods, and the complex food processing system overall begins to show the larger problem. It’s a system collapse by a thousand paper cuts.
Some well intentioned people will claim the shortage of processed and manufactured food is a good thing, and people should eat more fresh foods and be healthier.
Let me be very frank about this. Without full-service fresh prepared food delivery operating normally (restaurants, hotels, cafeterias, lunchrooms, food trucks, venues etc) there isn’t enough fresh food in the U.S. retail distribution system (grocery chains) to feed 350 million people.
We simply need processed and manufactured foods.
Additionally, many of those manufactured foodstuffs (spices, sauces, etc) are additives to what people call “fresh food” preparation. If you want salt, pepper, olive oil, butter, tomato paste, pasta, flour, etc., you need processed and manufactured food.
As we go into this phase, the ABC report was correct on where these issues will be less noticeable, less fragile. The smaller grocery outlets with closer connections to the field. The closer the grocer is to the farmer, the less fragile they are in this shortage phase. “Grocers” (traditionally defined) will do better than “supermarkets”.
Also think about it like this. Does your grocery store have an in-store bakery? If so, their ability to make bread means they are less susceptible to running out of bread. If processed industrial bakeries experience issues, your in-store bakery may not. You will pay much more, but the product will exist. The key is having knowledge of where the product exists.
On a supermarket basis, the total operational excellence comes into play now. Top shelf field-to-fork operations like Hannaford, HEB, Publix and Wegmans will fare much better than Kroger, Ahold, Giant Eagle, Albertsons, Shop Rite, Meijer, Safeway, Winn Dixie etc. You can see how the former group rely more on fresh product supply chain relationships, and the latter group are weighted heavily toward low-price highly manufactured.
Posted originally on the conservative tree house on January 16, 2022 | Sundance | 157 Comments
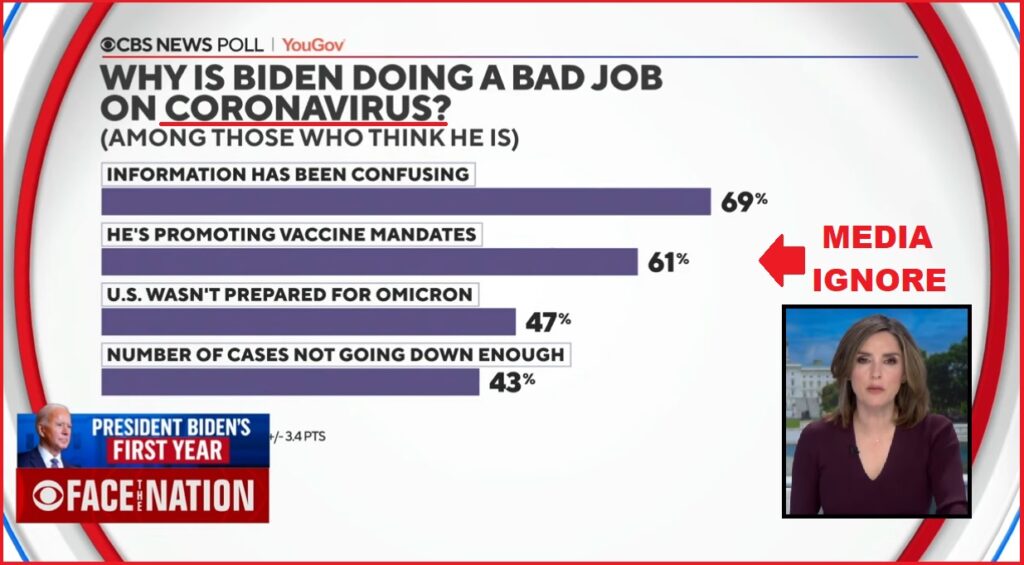
CBS conducted a poll of the collapsed support for Joe Biden [DATA HERE] and then outlined their findings earlier today. However, keeping up with their need to ignore things, they skip over how the vaccination mandate is opposed within their responses.
Margaret Brennan and Anthony Salvanto, CBS News’ director of elections and surveys, discuss how inflation and the economy are the two central issues at the top of concern. However, Joe Biden’s handling of COVID, and specifically the vaccination mandate, are also driving opposition to the regime intent. WATCH:
The people behind Biden have boxed him in on the economic consequences. Inflation is an outcome of economic policy that cannot be reversed without completely refuting their own policy and reversing course. As a consequence, there’s nothing Biden can do to stop this negative outcome.
That said, notice the aspect in the screengrab below (polling outcome) which they completely ignored.
A few people have questioned my comment on Virginia Giuffre saying she was a victim of sex trafficking. I totally disagree. Just watch the movie Taken which is based on the real sex trafficking trade. There they kidnap girls who are then forced to have sex. That by no means applies to what Epstein was doing. He enticed girls into a high-level standard of living and they were trained how to have sex. They voluntarily joined that lifestyle which is substantially different from the girls who are really victims of the sex trade. I do not think it is appropriate to lump them all together into one group. The sex trade is a serious issue. I have always advised even our staff never to walk alone in the major cities of London, Paris, or Rome. They even have been kidnapping them in New York City. With this defunding of the police, it will only get worse. This is also unfolding in California.
Posted originally on the Conservative tree house on January 15, 2022 | sundance | 57 Comments
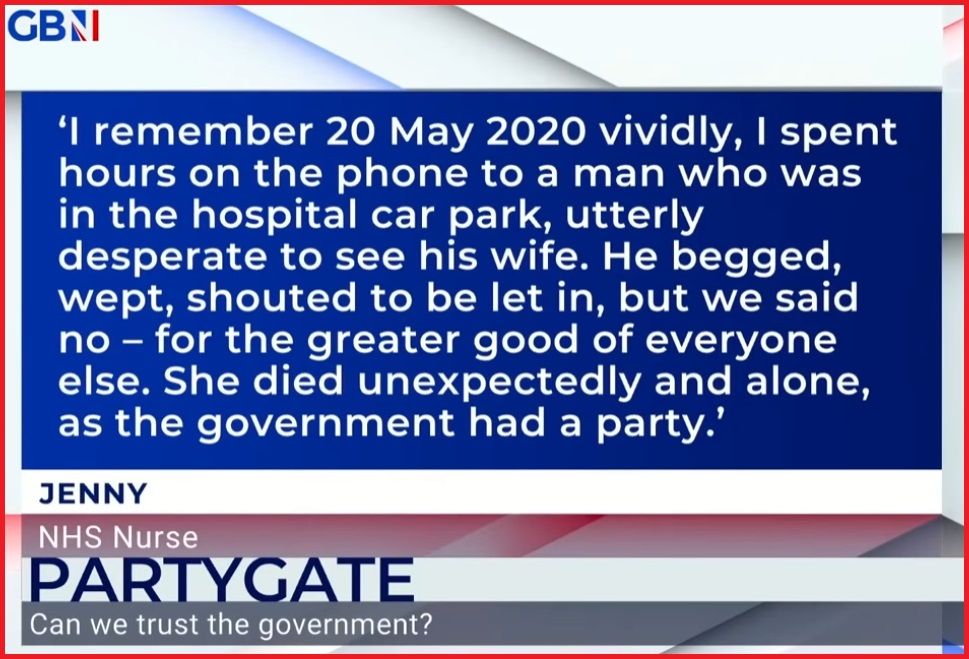
Neil Oliver does a weekly monologue that is very well articulated and provokes thought; this one is no exception.
In this outline Oliver weaves a series of points around the topic of collapsed trust with government and institutions with examples we all relate to. However, the last 90-seconds, when he connects them is brilliant, painful and disturbing. Highly recommended.
That final example is enough to make us weep in anguish, and then anger.
Posted originally on the conservative tree house on January 15, 2022 | sundance | 348 Comments
There has been a great deal of discussion and debate about the Democrat party having evolved into a full-blown communist apparatus. However, a Rasmussen poll released today [DATA HERE] puts the debate to rest with empirical data.
Democrats are FACTUALLY the party of totalitarian communists. Consider:
♦ Forty-five percent (45%) of Democrats favor the government forcing unvaccinated people into federal quarantine camps if they refuse the COVID-19 vaccine.
♦ Nearly half (48%) of Democrat voters think federal and state governments should be able to fine or imprison individuals who publicly question the efficacy of the existing COVID-19 vaccines on social media, television, radio, or in online or digital publications.
♦ 47% of Democrats favor a government tracking system, ankle monitors or locked collars, for those who won’t get the COVID-19 vaccine.
♦ Twenty-nine percent (29%) of Democratic voters support forcibly removing children from the custody of unvaccinated parents.
♦ 55% of Democratic voters support fines and financial punishment for the unvaccinated.
♦ Fifty-nine percent (59%) of Democrats favor government requiring unvaccinated citizens to remain confined to their homes. (read poll here)
Posted originally on the conservative tree house on January 15, 2022 | sundance | 272 Comments
I saw this last night and was actually a little taken back in the exchange. For some unknown reason (though I have suspicions), instead of Alex Berenson using his time on Fox News to confront the malicious and fraudulent manipulation of medical science, he decided to attack the credibility of Dr. Robert Malone.
There could be nefarious motives for this; however, the Occam’s Razor perspective is simply that Alex Berenson carries a thin-skinned trait of social awkwardness and is unaware how his engagements with people can be off-putting. You decide. WATCH:
Posted originally on the conservative tree house on January 15, 2022 | sundance | 187 Comments
Comrades, when we permit the government to gather private cell phone data, the government will always gather private cell phone data. In Canada the health officials have now admitted they captured, without legislative authority, the personal cell phone data and geolocation data of 33 million Canadians.
As a result, and a little late all things considered, privacy issues are being raised about the Public Health Agency of Canada (PHAC) buying the location data of Canadian cellphone users to monitor their activity. The agency said it wanted to analyze the movement of people during the pandemic to ensure their safety and well-being.
However, the implications of a totalitarian administrative state monitoring citizens under the guise of pandemic authority, does not make everyone feel comfy. John Brassard, a conservative member of parliament, questions the pandemic surveillance and legal authority. WATCH:
They are only secretly monitoring you for your health comrades, promise.
Byram W. Bridle, PhD, MSc, Associate Professor of Viral Immunology, Department of Pathobiology, University of Guelph, Guelph, ON, Canada, bbridle@uoguelph.ca
Bonnie A. Mallard, PhD, Professor of Immunogenetics, University of Guelph, Guelph, ON, Canada, bmallard@uoguelph.caSubscribe to the Trialsitenews “COVID-19” ChannelNo spam – we promise
Niel A. Karrow, PhD, MSc, Associate Professor, Department of Animal Biosciences, University of Guelph, Guelph, ON, Canada, nkarrow@uoguelph.ca
David J. Speicher, PhD, MSc, Senior Research Associate, Department of Pathobiology, University of Guelph, Guelph, ON, Canada, research@davidspeicher.com
Claudia Chaufan, MD, PhD, Associate Professor of Health Policy and Global Health, York University, Toronto, ON, Canada, claudia.chaufan@protonmail.com
Julian G.B. Northey, PhD, MSc, Adjunct Professor, Ontario Tech. University, Oshawa, ON, Canada, julian.northey@utoronto.ca
Steven Pelech, PhD, Professor, Department of Medicine, University of British Columbia, Vancouver, BC, Canada, spelech@mail.ubc.ca
Christopher A. Shaw, PhD, Professor, Department of Ophthalmology and Visual Sciences, University of British Columbia, Vancouver, BC, Canada, cashawlab@gmail.com
Ondrej Halgas, PhD, MSc, Biomedical Researcher, University of Toronto, Toronto, ON, Canada, ondrej.halgas@mail.utoronto.ca
Deanna McLeod, HBSc, Principal and Lead, Kaleidoscope Strategic, deanna@kstrategic.com
Citation: Bridle BW, Martins I, Mallard BA, Karrow NA, Speicher DJ, Chaufan C, Northey, JGB, Pelech S, Shaw CA, Halgas O, McLeod D. Concerns regarding the efficacy and safety for BNT162b2 mRNA coronavirus disease (COVID-19) vaccine through six months. http://www.CanadianCovidCareAlliance.org (January 10, 2022) 1-10.
Summary of concerns
Efficacy
• Important limitations of the stated efficacy claims were not discussed
• Only the relative risk reductions were stated; absolute risk reduction metrics were not presented
• Integration of adult and adolescent cohorts with differing follow-up periods were presented without explanation
• Large number of discontinued or missing participants comparable to primary end-point event numbers
• Prior SARS-CoV-2 infections screened only in a subset of trial participants, and determined only by an antibody test with severe sensitivity limitations
• Cut-offs of the RT-PCR positivity tests were not reported; no confirmatory functional virology assays were performed
• Absence of systematic testing and unbiased testing framework for the detection of SARS-CoV-2-infected participants
Safety
• Trial participants were healthier than the average population
• Monitoring of adverse events were limited in time and scope
• Number of severe adverse events in the vaccine arm were much higher than the numerical reduction in severe COVID-19 cases between vaccine and placebo arms
• Superficial evaluation of the most clinically relevant end-point – survival; no independent assessment of the causes of death provided
• Cardiovascular adverse vaccine events are now widely recognized, yet no systematic monitoring of cardiovascular health was carried out
• Substantially higher number of solicited and unsolicited adverse events, most of which presented as COVID-19-like symptoms, in the vaccine arm yet study claims efficacy against symptomatic COVID-19
• Increase in cardiac-related deaths in the vaccine arm compared to placebo arm
• Inability to assess long term safety within the trial due to unblinding and participant crossover to the vaccine arm
Other concerns
• Multiple conflicts of interest of a large majority of study authors
• Multiple trial irregularities reported by Thacker et al. (1) published in the British Medical Journal
Article
We present several concerns regarding the recent article by Thomas et al. (2) on the efficacy and safety of the BNT162b2 mRNA coronavirus disease (COVID-19) vaccine, which was published in the New England Journal of Medicine (NEJM) on November 4, 2021. An abbreviated version of this letter was submitted to the NEJM on November 15, 2021 and declined for publication on November 29, 2021 due to limited space. The study assessed the BNT162b2 in individuals that were healthy or had stable chronic medical conditions and concluded that, “through 6 month follow up, despite a gradual decline in vaccine efficacy, BNT162b2 had a favorable safety profile and was highly efficacious at preventing COVID-19.” We present numerous concerns regarding the reported safety and efficacy of this injection.
Efficacy
First, Thomas et al. (2) reported BNT162b2 efficacy as a relative risk reduction of contracting symptomatic reverse-transcriptase-polymerase chain reaction (PCR)-confirmed COVID-19 of 91.3% (77 vs 850 cases) and severe symptomatic PCR-confirmed COVID-19 of 96.7% (1 vs 30 severe cases). Thomas et al. (2) should have reported efficacy as an absolute risk reduction as per the communicating risks and benefits guidelines issued by the United States Food and Drug Administration (FDA) (3), which would have highlighted the modest absolute risk reductions provided by the vaccine in both symptomatic (3.7%) and severe symptomatic (0.7%) PCR-confirmed COVID-19.
Second, this analysis is the only published account of the BNT162b2 phase I – III trial efficacy outcomes among adults ≥16 years of age through six-month follow-up after immunization. In a trial amendment, a cohort of adolescents aged 12 to 15 years was added to the phase III study for which there was a shorter follow-up period. In this analysis, Thomas et al. (2) combined the two cohorts in providing efficacy outcomes after a six month follow up and departed from the initial analysis without providing a reasonable explanation for doing so. Given that vaccine efficacy wanes over time, by combining the older and younger cohorts, Thomas et al. (2) obfuscated the efficacy of the older group at six months. The authors should have provided efficacy outcomes for both groups and explicitly state the two reporting time periods in their conclusion.
Third, when discussing their findings, Thomas et al. (2) did not mention that a larger proportion of participants in the placebo group discontinued the trial compared to the vaccine group; 40% more after the first dose (271 vs 380 participants) and 63% more after the second dose (167 vs 273 participants). Discontinuations consisted mostly of “voluntary withdrawals”, “no longer meeting the eligibility criteria” and “lost to follow-up.” Additionally, there were a high number of participants missing from the CONSORT diagram between 2nd dose and the open-label period with more participants missing in the vaccine arm (1,258 vs 583 missing). These imbalances, which were in the order of the number of primary end-point events (77 and 850, for vaccine and placebo, respectively) call into question the reliability of these findings. Thomas et al. (2) should have disclosed the details related to the nature of these losses and discussed the impact they may have had on overall findings.
Fourth, Thomas et al. (2) used inappropriate tests when assessing current or prior infections due to severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2). The authors screened 10,453 serum samples for COVID-19 infections up to 6 weeks prior to enrollment using the Roche Elecsys® Anti-SARS-CoV-2 antibody test, which tests for only the nucleocapsid protein of SARS-CoV-2 and has high sensitivity 14 days after infection when antibodies tend to peak (4). However, as antibody levels wane over time despite persisting immunity, it is unlikely that this test alone could identify prior immunity to SARS-CoV-2 or distinguish between prior immunity to other coronaviruses, which express similar proteins. Additionally, testing for the SARS-CoV-2 was done with the Cepheid Xpert Xpress SARS-CoV-2 RT-PCR rather than the gold-standard functional virology assay, looking for cytopathic effect in permissive cells. FDA specifications for PCR testing at that time the trial was conducted tended toward cycle thresholds beyond 20-30 cycles (5), which are now widely recognized as being unreliable in detecting an active COVID-19 infection (6-8). Given these limitations, Thomas et al. (2) should have used better screening for natural immunity, used a functional virology assay, and discussed the implications of these testing limitations in their findings.
Fifth, we noted an absence of systematic testing and an objective testing framework for the detection of SARS-CoV-2-infected participants. In this study, it was left to the discretion of the investigator to send a patient presenting with COVID-19-like symptoms for laboratory confirmation of SARS-CoV-2 infection, a task which would be particularly difficult given that reactogenicity events consisted principally of COVID-19-like symptoms (Thomas et al. (2), Figure S1). This lack of systematic testing introduced a concerning level of variability and subjectivity associated with the identification of both symptomatic cases and disease severity (9,10). Thomas et al. (2) should have discussed the implications of this lack of objective and systematic virological assessment on their study findings as well as presented data related to asymptomatic testing that was conducted at “selected sites.” Overall, the emphasis on relative risk reductions, the combining efficacy outcomes from the adult and adolescent cohorts, the large number of people who were excluded from the analysis, and the use of inappropriate tests and lack of objective testing framework call into question the authors’ conclusions regarding vaccine efficacy.
Safety
First, Thomas et al. (2) concluded their article by stating that BNT162b2 showed a “favorable safety profile,” and in their abstract stated that “BNT162b2 continued to be safe and have an acceptable adverse-event profile.” However, Thomas et al. (2) Figure S1 summarized solicited adverse events reported within 7 days of the first dose in the reactogenicity subset, which represented a mere 22% of the randomized population. A considerably higher rate of local and systemic adverse events was reported among vaccine recipients with a marked increase in adverse events with the second dose. The preponderance of systemic effects in both arms were COVID-19-like symptoms and occurred at higher rates than in the vaccine compared to the placebo group, despite the vaccine group having a higher number of identified symptomatic COVID-19 cases (77 vs 850, vaccine vs placebo, respectively). The very need for this trial is predicated on the importance and clinical relevance of eradicating COVID-19 symptoms. How is it then that such consistent increases in COVID-19-like symptoms among vaccine recipients are described as “favorable”?
Second, Thomas et al. (2) provided a descriptive analysis of vaccine safety. To better compare the benefits and the risks of this vaccine, we calculated absolute and relative risk reductions/increases (ARR/ARI and RRR/RRI, respectively) associated with the vaccine for efficacy events seven days after the second dose (i.e., corresponding to full vaccination for those in the vaccine group) and for safety events during the respective data collection period (starting with the first-dose). These calculations were based on the eligible population for each relevant safety and efficacy events without adjusting for surveillance time as that data was not published for safety events. A simple chi-square calculator was used to assess the significance of the difference in event numbers between groups (Table 1) (11).
Table 1. Differences in the number of efficacy and safety events in eligible populations¥ reported in the 6-month update of the BNT162b2 mRNA Covid-19 vaccine
Event
BNT162b2(n)
Placebo(n)
Absolute Difference (p-value)?
Absolute Risk Change* (%)
Relative Risk Change* (%)
Cases Adults and Adolescents 7 days after 2nd dose$
77
850
-773 (p<0.00001)
-3.7
-90.9
Any Unsolicited Treatment-Related Adverse Event Adults#
5,241
1,311
+3,930 (p<0.00001)
+17.9
+299.7
Any Severe Event Adults/
390
289
+101 (p=0.0001)
+0.5
+34.9
Severe Cases in Adults 7 days after 2nd dose&
1
23
-22 (p<0.00001)
-0.1
-95.7
Unsolicited Severe Adverse Events~ AdultsPrevents daily routine activity or requires intervention or worse
262
150
+112 (p<0.00001)
+0.5
+74.6
Serious Adverse Event Adults§Requires hospitalization or results in permanent injury or death
127
116
+11(p=0.5)
+0.05
+9.5
Deaths during placebo-controlled period [additional deaths during open-label period in vaccine recipients or placebo-only]%
15 [+5]
14 [NR]
+1 [+5](p=0.9)
+0.005
+7.1
Deaths due to cardiovascular events^
9
5
+4
¥ For the purpose of this table and in accordance with the terminology used in the study report, adult and adolescent populations are defined as ≥16 years old and 12-15 years old, respectively.
? Significance figures (p-values) estimated using chi-square calculator available at https://www.socscistatistics.com/tests/chisquare. P-values are without the Yates correction. This procedure was applied following the framework used by Classen (11) in his analysis of “All Cause Severe Morbidity” based on data from the initial reports of the vaccine Phase III trials
* Authors estimated vaccine efficacy using total surveillance time as denominator, however, as this value was unavailable for all the events analyzed, our calculations used the common statistical definition, i.e., number of events relative to total number of eligible patients for each event analysis reported29 similar to previous analyses of this nature (11-30);
$ ≥7 Days after dose 2 among participants without evidence of previous infection
# Adverse events reported outside of the reactogenicity subgroup and assessed by the investigator as related to investigational product
/ In calculations combining efficacy and safety events, the number of patients randomized that received any dose of vaccine or placebo was used as the study population in the statistical calculations, following the framework used by Classen (11) in his analysis of “All Cause Severe Morbidity”. Differences in the total (event-incident) population (randomized vs efficacy vs safety) used as denominator are relatively small and are expected to have minimal impact on the relative differences between groups. Without access to individual patient data, these calculations were performed under the assumption that efficacy and safety events were non-overlapping
& ≥7 Days after dose 2; confirmed severe COVID-19 defined as PCR-positivity and “presence of at least one of the following: • Clinical signs at rest indicative of severe systemic illness (RR ≥30 breaths per minute, HR ≥125 beats per minute, SpO2 ≤93% on room air at sea level, or PaO2/FiO2 <300 mm Hg); • Respiratory failure (defined as needing high-flow oxygen, noninvasive ventilation, mechanical ventilation, or ECMO); • Evidence of shock (SBP <90 mm Hg, DBP <60 mm Hg, or requiring vasopressors); • Significant acute renal, hepatic, or neurologic dysfunction;• Admission to an ICU; • Death”
~ Severe (grade ≥3) adverse events were generally defined as those that interfere significantly with participant’s usual function, those that affect daily living or require medical care; grade 4 events were generally defined as those that required emergency room visit or hospitalization
§Serious adverse events were defined as any untoward medical occurrence that, at any dose: a. Results in death; b. Is life-threatening; c. Requires inpatient hospitalization or prolongation of existing hospitalization; d. Results in persistent disability/incapacity.
% Deaths during the open-label period were reported only in vaccine recipients, 3 participants in the BNT162b2 group and 2 in the original placebo group who received BNT162b2 after unblinding
^Those with reported cause of death due to: aortic rupture, arteriosclerosis, cardiac arrest, cardiac failure congestive, cardiorespiratory arrest, hypertensive heart disease, or myocardial infarction
Our findings showed that the increase in unsolicited adverse events in vaccine recipients, which included at least one adverse event up to 1 month post the second dose, was greater (RRI of 299.7% and ARI of 17.9%; p<0.00001) than the reduction in identified symptomatic COVID-19 cases observed in fully-vaccinated individuals for the duration of the trial (RRR of 90.9% and ARR of 3.7%; p<0.00001).
A similar pattern was observed for severe and serious adverse events. The study concluded that “vaccine efficacy against severe disease was 96.7%.” However, our analysis showed that the vaccine was associated with a significant increase in severe adverse events defined as an adverse event that interferes significantly with daily activity or requires medical care (RRI of 74.6% and ARI of 0.5%; p<0.00001) and a numerical increase in serious adverse events, defined as any untoward medical occurrence that was life-threatening, required hospitalization or resulted in persistent disability up to 6 months (RRI of 9.5% and ARI of 0.05%; p=0.5) compared to placebo. These increases were greater than the reduction in severe COVID-19 cases observed in fully-vaccinated individuals for the duration of the trial (RRR of 95.7% and ARR of 0.1%; p=0.00002). When severe COVID-19 events were pooled with severe or serious adverse events to determine the likelihood of experiencing any severe event (11), there was an overall increase in severe events among vaccine recipients compared with placebo (RRI of 34.9% and ARI of 0.5%, p=0.0001). Given these findings, Thomas et al. (2) should have revised their conclusion to state, “the vaccine was associated with a concerning and clinically meaningful increase in severe events relative to placebo.”
Third, Thomas et al. (2) conducted minimal monitoring of adverse events (12). Firstly, the solicited reactogenicity data was collected for only a small portion of trial participants (9,839/44,047 or 22.3%), for a limited 7 days after each dose, and for only a short pre-specified list of systemic and injection site reactions with no monitoring of sub-clinical effects. Secondly, unsolicited adverse events were collected for a mere 1 month and serious adverse events for only 6 months following the second dose. This means that severe vaccine related cardiac, neurological or immunological injuries that took more than a month to diagnose and were not considered serious, would not be reflected in the findings. Thirdly, unblinding and subsequent crossover of those on the placebo arm to the vaccine arm, will certainly attenuate any safety signals coming from this trial as well as preclude insights into long-term safety which were to be monitored for 2 years. Thomas et al. (2) should have commented on the implications their abbreviated monitoring schedule may have on safety underreporting as well as the implications of unblinding on short- and long-term safety outcomes. Given the increase in severe events (RRI of 34.9% and ARI of 0.5%) and cardiovascular deaths associated with the vaccine (n= 9 vs 5, vaccine vs placebo, respectively), The authors should have more closely monitored safety and provided a detailed discussion of the severe and serious adverse events along with a discussion of their potential long-term implications.
Fourth, given the inclusion of adolescents and “healthy participants who had stable chronic medical conditions” in the study population, we noted very little discussion of death, the most clinically relevant end-point of this trial. Thomas et al. (2) Table S3 showed a slightly higher number of deaths in the vaccine group (n=15 vs n=14 in the placebo group during the blinded period). However, the manuscript text (Thomas et al. (2), page 7) stated that five additional deaths occurred in vaccine recipients after unblinding (two of which were initially allocated to the placebo group) for a total of 20 deaths in vaccine recipients. Thomas et al. (2) Table S4 also showed that although only 3 study deaths were attributed to COVID-19 or COVID-19 pneumonia (n=1 vs n=2, vaccine vs placebo, respectively) a total of 14 deaths were cardiovascular in nature (aortic rupture, arteriosclerosis, cardiac arrest, cardiac failure congestive, cardiorespiratory arrest, hypertensive heart disease) with the almost twice as many occurring in the vaccine arm (n=9 vs n=5, vaccine vs placebo, respectively). There is currently an abundance of real-world evidence to support an association between cardiovascular adverse events and the vaccines (13-17). Thomas et al. (2) reported that “none of these deaths were considered to be related to BNT162b2 by the investigators” without describing the objective framework of testing that allowed them to arrive at that conclusion or whether their findings were independently evaluated. Given the seriousness of these adverse events in an otherwise healthy population, Thomas et al. (2) should have provided a detailed description of how they arrived at their conclusion, these evaluations should have undergone independent assessment, and all ongoing study protocols investigating BNT162b2 should be immediately amended to include systematic short- and long-term clinical and sub-clinical monitoring of cardiovascular health. Overall, the increased rates of COVID-like symptoms, unsolicited adverse events as well as severe and serious adverse events in the vaccine compared to the placebo arm, as well as the net increase in deaths in vaccine recipients compared with those who were unvaccinated present serious concerns regarding the safety of these biological agents.
Conflicts of Interest
The disconnect between author conclusions, our analysis of the data, and the NEJM rejection of our letter to the editor led us to examine author disclosures for potential conflicts of interest (COI) (Table 2). Our analysis revealed multiple direct conflicts of interest. The article was supported by BioNTech and Pfizer, the corresponding author, Judith Absolon, and the senior author, Kathrin Jansen were employees of Pfizer and owned company stock, and the first author Stephen Thomas was a consultant to Pfizer. Of the 32 authors, 21 (66%) were employees of Pfizer or BioNtech and 26 (81%) had Pfizer/BioNtech-related conflict of interests. We also noted that one of NEJM’s senior editors is also a co-principal investigator of the related Moderna-Vaccine COVE-trial (18,19).
Table 2. Conflicts of interest related to Pfizer/BioNTech
Title
Author
Corresponding author
Judith Absalon: Pfizer employment and stock holder
First author
Stephen Thomas: Pfizer consultancy
Last author
Kathrin Jansen: Pfizer employment and stock holder
Other 29 authors (66% employees, 81% had some COI)
Pfizer/ BioNTech employment and stockholder, n=15; Pfizer/ BioNTech employment (without stock) n=4; Pfizer grant/contract n=3; Pfizer clinical trial n=1; Other company consultancy n=1; No COI n=5
Conclusion
Our critique of the Thomas et al. (2) publication revealed multiple concerns regarding author claims of BNT162b2 safety and efficacy as well as a high number of direct conflicts of interest in the publication authors. These, coupled with multiple reports indicating that vaccine efficacy wanes within months of administration (20-23), reduced effectiveness of BNT162b2 with respect to emerging variants (24-26), record rates of serious adverse events (122,833) and deaths (17,128) reported in the US passive Vaccine Adverse Event Reporting System, VAERS by October 16, 2021, and problems with data integrity in the conduct of this trial reported recently by Thacker (1) in the British Medical Journal, raise further concerns regarding both the efficacy and safety of this agent. We did not find sufficient evidence to support use of these agents in the healthy adults studied or in specific unstudied demographics that are being mandated to comply with vaccination including the naturally immune, the frail elderly, those with multiple co-morbidities, the immunocompromised, and pregnant women. It also calls into question use in adolescents and children given that companion trials conducted in those populations suffered from similar design flaws, including underpowered in participant numbers and that recommendations for use were based on minimal safety follow up (27,28).
Conflicts of Interest
Byram W. Bridle received funding from the Ontario Government (COVID-19 Rapid Research Fund, Ministry of Colleges and Universities) and Government of Canada (Pandemic Response Challenge Program, National Research Council of Canada) to conduct pre-clinical research with COVID-19 vaccines
Ilidio Martins, none to disclose
Claudia Chaufan, none to disclose
Julian Northey, none to disclose
Niel A. Karrow, none to disclose
Steven Pelech is the majority shareholder and president and Chief Scientific Officer of Kinexus Bioinformatics Corporation, which has been developing serological tests for detection of antibodies against SARS-CoV-2 proteins and testing of drugs to inhibit SARS-CoV-2 replication
Bonnie Mallard, none to disclose
Christopher A. Shaw has been an expert witness in Vaccine Court twice
David Speicher, none to disclose
Ondrej Halgas, none to disclose
Deanna McLeod, none to disclose
References
1. Thacker PD. COVID-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial. BMJ 2021;375:n2635.
2. Thomas SJ, Moreira ED, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine through 6 months. N Engl J Med 2021;385:1761-73.
3. Fischhoff B. Communicating risks and benefits: An evidence based user’s guide. Silver Spring, MA, USA: Food and Drug Administration (FDA), US Department of Health and Human Services. Government Printing Office; 2012.
5. Cepheid. Xpert® Xpress SARS-CoV-2 – Instructions for use. For use under an Emergency Use Authorization (EUA) only. U. S. Food and Drug Administration, 2021. (Accessed June 29, 2021, at https://www.fda.gov/media/136314/download.)
6. Mina MJ, Peto TE, García-Fiñana M, Semple MG, Buchan IE. Clarifying the evidence on SARS-CoV-2 antigen rapid tests in public health responses to COVID-19. The Lancet 2021;397:1425-7.
7. Al Bayat S, Mundodan J, Hasnain S, et al. Can the cycle threshold (Ct) value of RT-PCR test for SARS CoV2 predict infectivity among close contacts? Journal of Infection and Public Health 2021;14:1201-5.
11. Classen B. US COVID-19 vaccines proven to cause more harm than good based on pivotal clinical trial data analyzed using the proper scientific endpoint,“All cause severe morbidity”. Trends Int Med 2021;1:1-6.
13. Rose J. A Report on the US Vaccine Adverse Events Reporting System (VAERS) of the COVID-19 messenger ribonucleic acid (mRNA) biologicals. Sci, Pub Health Pol, & Law 2021;2:59-80.
14. Kaur RJ, Dutta S, Charan J, et al. Cardiovascular adverse events reported from COVID-19 vaccines: A study based on WHO database. Int J Gen Med 2021;14:3909.
15. Aye YN, Mai AS, Zhang A, et al. Acute myocardial infarction and myocarditis following COVID-19 vaccination. QJM: monthly journal of the Association of Physicians 2021.
16. Diaz GA, Parsons GT, Gering SK, Meier AR, Hutchinson IV, Robicsek A. Myocarditis and pericarditis after vaccination for COVID-19. JAMA 2021;326:1210-2.
17. Barda N, Dagan N, Ben-Shlomo Y, et al. Safety of the BNT162b2 mRNA COVID-19 vaccine in a nationwide setting. N Engl J Med 2021;385:1078-90.
18. Baden LR, El Sahly HM, Essink B, et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med 2021;384:403-16.
19. Keil U. Re: COVID-19: How independent were the US and British vaccine advisory committees? BMJ 2021;373:n1283. 2021. (Accessed Dec 6, 2021, at Re: COVID-19: How independent were the US and British vaccine advisory committees?)
20. Goldberg Y, Mandel M, Bar-On YM, et al. Waning immunity after the BNT162b2 vaccine in Israel. N Engl J Med 2021.
21. Puranik A, Lenehan PJ, O’Horo JC, et al. Durability analysis of the highly effective BNT162b2 vaccine against COVID-19. medRxiv 2021.
22. McDade TW, Demonbreun AR, Sancilio A, Mustanski B, D’Aquila RT, McNally EM. Durability of antibody response to vaccination and surrogate neutralization of emerging variants based on SARS-CoV-2 exposure history. Sci Rep 2021;11:1-6.
23. Andrews N, Tessier E, Stowe J, et al. Vaccine effectiveness and duration of protection of Comirnaty, Vaxzevria and Spikevax against mild and severe COVID-19 in the UK. medRxiv 2021.
24. Collie S, Champion J, Moultrie H, Bekker L-G, Gray G. Effectiveness of BNT162b2 vaccine against Omicron variant in South Africa. N Engl J Med 2021.
25. Lefèvre B, Tondeur L, Madec Y, et al. Beta SARS-CoV-2 variant and BNT162b2 vaccine effectiveness in long-term care facilities in France. The Lancet Healthy Longevity 2021;2:e685-e7.
26. Hansen CH, Schelde AB, Moustsen-Helm IR, et al. Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study. medRxiv 2021:2021.12.20.21267966.
27. Frenck RW, Jr., Klein NP, Kitchin N, et al. Safety, immunogenicity, and efficacy of the BNT162b2 COVID-19 vaccine in adolescents. N Engl J Med 2021;385:239-50.
28. Walter EB, Talaat KR, Sabharwal C, et al. Evaluation of the BNT162b2 COVID-19 vaccine in children 5 to 11 years of age. N Engl J Med 2021.
I have created this site to help people have fun in the kitchen. I write about enjoying life both in and out of my kitchen. Life is short! Make the most of it and enjoy!
This is a library of News Events not reported by the Main Stream Media documenting & connecting the dots on How the Obama Marxist Liberal agenda is destroying America