This research also includes a groundbreaking study to determine the lethality of Covid-19 based on the most comprehensive available measure: the total years of life that it will rob from all people. This accords with the CDC’s tenet that “the allocation of health resources must consider not only the number of deaths by cause but also” the “years of potential life lost.”
The CDC emphasizes that the Covid-19 pandemic “is a rapidly evolving situation,” and as such, the emboldened figures in this article will be updated each weekday as the CDC publishes new data.
On one hand, the facts show that:
- the death rate for people who contract Covid-19 is uncertain but is probably closer to that of the seasonal flu than figures commonly reported by the press.
- the average years of life lost from each Covid-19 death are significantly fewer than from common causes of untimely death like accidents and suicides.
- the virus that causes Covid-19 is “very vulnerable to antibody neutralization” and has limited ability to mutate, which means it is very unlikely to take masses of lives year after year like the flu and other recurring scourges.
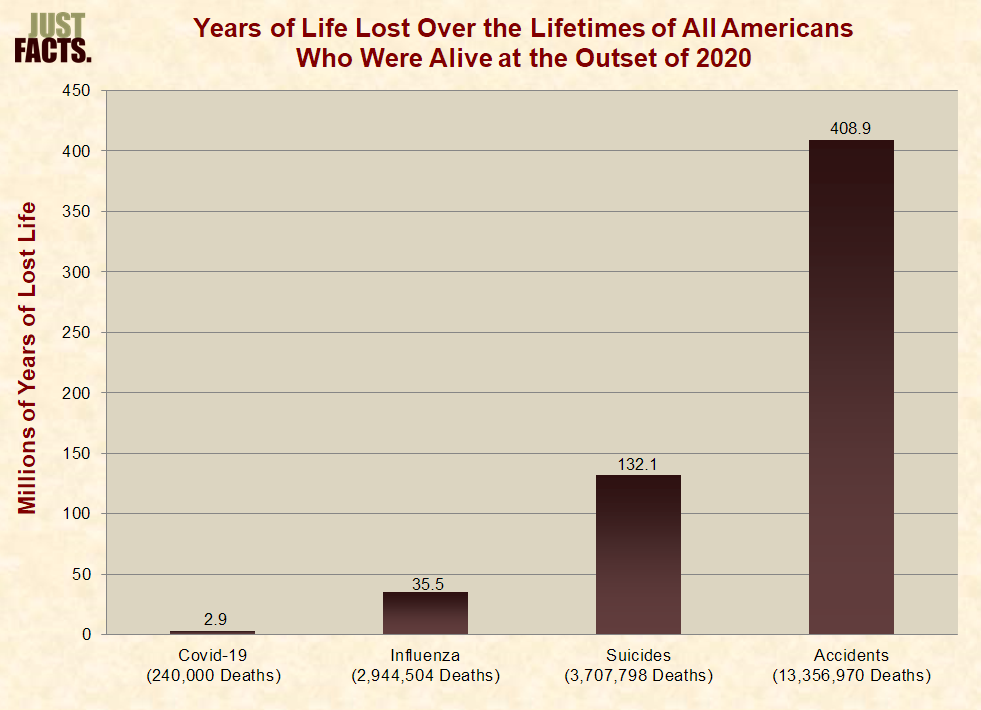
- if 240,000 Covid-19 deaths ultimately occur in the United States, the virus will rob about 2.9 million years of life from all Americans who were alive at the outset of 2020, while the flu will rob them of about 35 million years, suicides will rob them of 132 million years, and accidents will rob them of 409 million years.
(Source Data)
On the other hand, elderly people and those with chronic ailments are extremely vulnerable to Covid-19. Furthermore, the disease is highly transmissible, which means it could spread like wildfire and overwhelm hospitals without extraordinary measures to contain it. This would greatly increase its death toll.
However, such precautionary measures often have economic and other impacts that can cost lives, and overreacting can ultimately kill more people than are saved.
Per the U.S. Centers for Disease Control and Prevention, a total of 2,459,472 people in the United States have been diagnosed with Covid-19 as of 4:00 PM EST on June 26, 2020. The U.S. population is 330 million people, which means that one out of every 134 people has been diagnosed with Covid-19. The disease is not equally dispersed throughout the nation, so this figure is much higher in some areas and much lower in others.
Reported cases don’t include people who may have Covid-19 but have not yet been diagnosed. Because its incubation periodis 2–14 days, the number of people who have been infected could substantially exceed the number who have been diagnosed.
Also, the vast majority of people who contract Covid-19 experience only mild or no symptoms, and many of them may never be diagnosed. This means that the count of reported cases further understates the actual number of people who have been infected. A February 2020 study in the Journal of the American Medical Association based on data from China found that 81% of reported Covid-19 cases are “mild.” The true portion of such cases is even higher than this, for as the paper explains, there are “inherent difficulties in identifying and counting mild and asymptomatic cases.”
A rare case in which asymptomatic cases can be counted is the Diamond Princess cruise ship, since all passengers were tested for Covid-19. Among those who tested positive, 51% didn’t have symptoms when they were tested. The number of these people who later developed symptoms is currently unavailable.
In another such rare case, the New England Journal of Medicine reported in mid-April that universal Covid-19 testing of pregnant women at two New York City hospitals found that 88% of the women who tested positive for the disease were asymptomatic.
Conversely, the number of people who have ever been infected may greatly exceed the number who are still infected. Growing numbers of people who were once diagnosed with Covid-19 have recovered, and the count of those who were unknowingly infected and had fast recoveries could be enormous. A March 2020 paper in the journal Microbes and Infection notes that “most infected individuals … appear to be able to recover with little to no medical intervention.”
Moreover, a March 2020 paper in the Pediatric Infectious Disease Journal states: “Preliminary evidence suggests children are just as likely as adults” to contract Covid-19, but they are “less likely to be symptomatic,” and even those with diagnosed infections typically “recover 1–2 weeks after the onset of symptoms.”
The upshot of all this is that the number of people who are actively infected and contagious is lower than the total of reported and undiagnosed cases.
A March 2020 paper in the journal Science condenses the factors above into a single number. It estimates that 86% of all Covid-19 infections in Wuhan, China “were undocumented” before the government implemented travel restrictions. This means that the number of people who were infected was six times the number of documented infections. This figure declines as social distancing measures are adopted and as diagnoses and recoveries rise as time passes.
Under that worst-case scenario from Wuhan, if the number of people with contagious Covid-19 infections in the U.S. is actually six times the number of people who have been diagnosed with it, the average American would have to come in contact with 22 people to be exposed to one person who has it.
According to the CDC’s counts of “confirmed and probable” fatalities from Covid-19, a total of 124,976 U.S. residents have died from the disease as of 4:00 PM on June 26, 2020. To put this figure in perspective:
- Covid-19 has killed about one out of every 2,638 Americans, whereas one out of every 116 Americans die every year.
- roughly 12,469 people in the U.S. died from the swine flu from April 12, 2009 to April 10, 2010. Unlike Covid-19, which mainly kills older people with preexisting health problems, 87% of people killed by the swine flu were under the age of 65.
- an average of 37,000 people in the U.S. have died from influenza (“the flu”) each year over the past nine years.
- around 170,000 people per year in the U.S. die from accidents.
In other words, deaths from Covid-19 are now 60.3% of the annual fatalities from the flu and accidents. Although Covid-19 is a new disease and took its first reported life in the U.S. during late February, this comparison may substantially overstate the relative deadliness of Covid-19 because fatalities from accidents and the flu occur in droves every year, and this is unlikely for Covid-19.
The primary reason why the flu takes tens of thousands of lives every year is because the viruses that cause it mutate in ways that prevent people from becoming immune to them. Per the Journal of Infectious Diseases, “All viruses mutate, but influenza remains highly unusual among infectious diseases” because it mutates very rapidly, and thus, “new vaccines are needed almost every year” to protect against it. While much remains to be seen about the mutations of the virus that causes Covid-19, the early indications are that it will not mutate rapidly and become an ongoing scourge.
As detailed in a March 2020 paper in a molecular biology journal that cites Michael Farzan, co-chair of the Department of Immunology and Microbiology at Scripps Research, once a vaccine for Covid-19 is developed, it “would not need regular updates, unlike seasonal influenza vaccines” because the part of the virus that the vaccine targets “is protected against mutation” by a feature of its genetic material, or RNA.
The same point applies to naturally acquired immunity. People who get Covid-19 develop natural antibodies that protect against future infections of it. The physiology textbook The Human Body in Health and Illness explains that such immunity, which is called “active immunity,” is “generally long lasting.” The same applies to diseases like measles, mumps, rubella, and polio. If someone contracts these diseases, they rarely get them again, and furthermore, they are very unlikely to transmit them to others. Thus, these people become firewalls against the spread of these contagions.
Media outlets like The Atlantic, Vox, and Forbes have turned the truth of this matter on its head by confusing the general nature of coronaviruses with that of Covid-19. The habit of calling Covid-19 “the coronavirus” can be very misleading because there are different types of coronaviruses, and Covid-19 is caused by just one of them. Coronaviruses are a family of RNA viruses that includes some common cold viruses. These viruses tend to mutate rapidly, but Covid-19 does not share that trait. Per the same March 2020 paper cited just above, the virus that causes Covid-19 “does not mutate rapidly for an RNA virus because, unusually for this category, it has a proof-reading function” in its genetics.
Likewise, a February 19th editorial in the British Medical Journal about Covid-19 reports that the “genome data available so far show no unexpected mutation rate or signs of adaptation….”
Put simply, Covid-19 does not mutate nearly as much as the flu, and thus, it is far less likely to take lives regardless of acquired immunity and vaccines. If this proves true in the long run, as current evidence suggests it will, the lifetime risk of dying from Covid-19 is greatly overstated by comparing its ultimate death toll to yearly fatalities from the flu, accidents, suicides, and other frequent causes of death.
Beyond raw numbers of deaths, another crucial factor in measuring the deadliness of a public health threat is the ages of its victims. In the words of the CDC, “the allocation of health resources must consider not only the number of deaths by cause but also by age.” Hence, the “years of potential life lost” has “become a mainstay in the evaluation of the impact of injuries on public health.”
In this respect, Covid-19 is much less lethal than common causes of untimely death, such as accidents. The precise average age of death for Covid-19 fatalities is still unknown, but the vast majority of victims are elderly or have one or more chronic illnesses, as is the case with deaths from the flu and pneumonia.
Based on the CDC’s latest data for the age distribution of deaths, the average age of death for accidents is about 53.3 years, while for the flu and pneumonia, it is about 77.4 years. Using flu and pneumonia as a rough proxy for Covid-19, this disease robs an average of 12.0 years of life from each of its victims, as compared to 30.6 years of lost life for each accident. And again, accidents kill around 170,000 Americans per year, while Covid-19 is unlikely to have an ongoing high death toll because of its limited prospects for mutation.
In a March 29th comment that generated headlines in virtually every major media outlet, renowned immunologist Anthony Fauci told CNN’s Jake Tapper that “looking at what we’re seeing now, I would say between 100,000 and 200,000” Americans will die from Covid-19, but “I just don’t think that we really need to make a projection when it’s such a moving target that you can so easily be wrong and mislead people.” The next day, Dr. Fauci emphasized that those figures are based on a model, and “a model is as good as the assumptions that you put into” it.
A day later at a White House press conference, Dr. Deborah Birx, another world-renowned immunologist, presented a slide of model results based upon “five or six international and domestic modelers from Harvard, from Columbia, from Northeastern, from Imperial who helped us tremendously.” The model projects that 100,000 to 240,000 deaths will occur if Americans follow social distancing and hygiene guidelines. She added that “we really believe and hope every day that we can do a lot better than that because that’s not assuming 100% of every American does everything that they’re supposed to be doing, but I think that’s possible.”
If the high-end of that range comes to pass, and 240,000 U.S. residents die from Covid-19, this disease will rob 2.9 millionyears of life from all Americans who were alive at the outset of 2020. In comparison, the flu will rob them of about 35 million years and accidents will rob them of 409 million years.
These figures reveal that accidents are about 140 times more lethal to Americans than this worst-case scenario for Covid-19 given mitigation. Likewise, the flu is 12 times as lethal. This is a substantially more comprehensive measure of deadliness than the tally of lives lost during a year—or any other random unit of time—because it accounts for the entirety of people’s lives and the total years of life that they lose.
While not diminishing the value of any life, these facts speak to the efforts that society takes to save some lives versus others.
Initial media reports of a 2–3% mortality rate for Covid-19 are inflated, and the actual figure may be closer to that of the flu, which has averaged about 0.15% over the past nine years in the United States. A large degree of uncertainty surrounds this issue due to the same factor that prevents accurate counts of infections: unreported cases.
As explained by Dr. Brett Giroir—who has authored nearly 100 peer-reviewed scientific publications and serves as the Assistant Secretary for Health at the U.S. Department of Health and Human Services—the Covid-19 death rate is “lower than you heard probably in many reports” because the bulk of people who contract coronavirus don’t get seriously ill, and thus, many of them never get tested.
Giroir calls this a “denominator problem” because if you’re “not very ill, as most people are not, they do not get tested. They do not get counted in the denominator.” Giroir’s best estimate is that the mortality rate is probably “somewhere between 0.1% and 1%.” This “is likely more severe in its mortality rate than the typical flu” rate of 0.1% to 0.15%, “but it’s certainly within the range.”
Giroir’s estimate accords with a February 2020 commentary in the New England Journal of Medicine by Fauci and others:
If one assumes that the number of asymptomatic or minimally symptomatic cases is several times as high as the number of reported cases, the case fatality rate may be considerably less than 1%. This suggests that the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.
A prime example of how journalists misreport on this issue is a March 12th article in Business Insider by Andy Kiersz. In this piece, he compares the “death rates” of Covid-19 from the South Korean CDC to that of the flu from the United States CDC. Based on these numbers, he reports that “South Korea—which has reported some of the lowest coronavirus death rates of any country—still has a COVID-19 death rate more than eight times higher than that of the flu.”
What Kiersz and his editors fail to understand is that the denominator for the Korean rate is the number of “confirmed cases,” while the denominator for the U.S. rate is based on a “mathematical model.” The CDC clarifies how the model works by citing a study on swine flu, which multiplies “43,677 laboratory-confirmed cases” of the disease by 41 to 131 times to calculate the denominator for the death rate. In the authors’ words, they do this because confirmed cases are:
likely a substantial underestimate of the true number. Correcting for under-ascertainment using a multiplier model, we estimate that 1.8 million–5.7 million cases occurred, including 9,000–21,000 hospitalizations.
Put simply, Covid-19 death rates that are based upon reported or confirmed infections grossly undercount the number of people with the disease. This, in turn, makes the death rate seem substantially higher than reality.
The famous maxim that “there are six degrees of separation between everyone in the world” has changed in recent years due to social media. A 2014 paper in the journal Computers in Human Behavior finds that the “average number of acquaintances separating any two people” has declined from six to 3.9.
A 2011 paper in the American Journal of Sociology estimates that each American knows an average of 550 people. If 150 of these are mutual connections who already know each other, each American has about 220,000 friends of friends—and 88 million friends of friends of friends.
Thus, if everyone is sharing on social media about people they know who have been infected or killed by Covid-19, it can seem like the world is coming to an end. Yet, if people did the same for other deaths, each person would hear every yearabout an average of:
- 1,905 deaths among their friends of friends, and 761,844 deaths among their friends of friends of friends.
- 38 deaths from the flu and pneumonia among their friends of friends, and 15,075 such deaths among their friends of friends of friends.
- 6 deaths of people under the age of 65 from the flu and pneumonia among their friends of friends, and 2,385 such deaths among their friends of friends of friends.
In addition to social media, the press acts as another megaphone of Covid-19’s impacts. Because the U.S. is the third-most populous nation in the world, it is easy for journalists to create misleading impressions by focusing on certain events and ignoring the broader context of facts that surround them. This kind of crucial context is missing from much of the media’s coverage of Covid-19 and practically every other public policy issue.
Another important factor in weighing the risks posed by Covid-19 is its transmissibility, or how contagious it is. In this respect, Covid-19 is much more dangerous than the seasonal flu because it spreads very quickly and can overwhelm hospitals.
Scientists measure the contagiousness of diseases with a basic reproduction number, which is the average number of people who tend to catch a disease from each person who has it. This measure is an innate characteristic of the disease because it doesn’t account for actions that people take to prevent it. A February 2020 paper published in the Journal of Travel Medicine explains that any disease with a basic reproduction number above 1.0 is likely to multiply over time.
The same paper evaluates 12 studies of the basic reproduction number of Covid-19 in various nations and finds that they “ranged from 1.4 to 6.49,” with an average of 3.28 and a median of 2.79. Based on their analysis of these studies, the authors conclude that the basic reproduction number of Covid-19 will likely prove to be “around 2–3” after “more data are accumulated.”
In contrast, a 2014 paper in the journal BMC Infectious Diseases analyzes 24 studies of the seasonal flu and finds that the median result for the basic reproduction number is 1.28. The authors stress that the seemingly small difference between 1.28 and higher figures like 1.80 “represent the difference between epidemics that are controllable and cause moderate illness and those causing a significant number of illnesses and requiring intensive mitigation strategies to control.”
In other words, if the transmissibility of Covid-19 is as high as currently estimated, the aggressive measures that some governments, organizations, and individuals have taken to limit large gatherings and travel from areas with outbreaks will save many more lives than doing the same for common diseases like the flu. Because Covid-19 spreads so quickly, it can easily overwhelm hospitals and thereby prevent people from getting the care they would otherwise receive under normal circumstances.
There are, however, mortal dangers in overreacting because measures to limit the spread of Covid-19 often have economic impacts that can cost lives. As detailed in the textbook Macroeconomics for Today, countries with low economic growth“are less able to satisfy basic needs for food, shelter, clothing, education, and health.” These hazards can manifest quickly and over extended periods of time.
If certain industries adopted the social distancing extremes that many people have embraced, this would shut down food production and distribution, health care, utilities, and other life-sustaining services. Even under far more moderate scenarios where people who are not in these industries shun work, all of those necessities and many more aspects of modern life depend on the general strength of the economy. Thus, overreacting can ultimately kill more people than are saved.
The same applies to people who are flooding supermarkets to stockpile food, toilet paper, and other supplies. In doing so, they have often stood in close proximity to each other and touched the same items, which opens avenues to spread the disease. Panic buying also creates shortages that deprive typical consumers of provisions.
Likewise, panic can fuel suicides, which snuff out about 47,000 lives per year in the U.S. at an average age of 46 years old. Over a lifetime, that amounts to 132 million lost years of life—or 46 times the loss from Covid-19 if it ultimately kills 240,000 people.
The implications of overreacting to Covid-19 or any other potential hazard are aptly summarized in a teaching guidepublished by the American Society for Microbiology. This book explains why “the factors driving your concept of risk—emotion or fact—may or may not seem particularly important to you, yet they are” because “there are risks in misperceiving risks.”
Aggressive social distancing can extend the timeframe over which Covid-19 patients are infected and hospitalized, but it cannot by itself reduce those outcomes in the long run. This is because Covid-19 is so contagious that another outbreak will begin and quickly proliferate as soon as the distancing measures cease.
Hence, the Imperial College’s March 16th report on Covid-19 states that in order to “avoid a rebound in transmission,” policies of “population-wide social distancing combined with home isolation of cases and school and university closure” must “be maintained until large stocks of vaccine are available to immunize the population—which could be 18 months or more.”
Moreover, the report notes that the “more successful a strategy is at temporary suppression, the larger the later epidemic is predicted to be in the absence of vaccination, due to lesser build-up of herd immunity.” A 2012 paper in the journal PLoS One about “Immunity in Society” underscores the importance of that point by noting that:
when a sufficiently high proportion of individuals within a population becomes immune (either through prior exposure or through mass vaccination), community or “herd” immunity emerges, whereby individuals that are poorly immunized are protected by the collective “immune firewall” provided by immunized neighbors. In humans and other vertebrate communities … responses to a previously encountered pathogen are faster and stronger than those to a novel pathogen, and thus individuals are better at blocking its spread. [Emphasis added.]
Equally, if very few people are immune to a disease, they can transmit it to others instead of blocking it. Without a vaccine, the only way people can become immune to Covid-19 is by catching it and recovering. This means that too much social distancing may cause more deaths because young, healthy people—who would otherwise catch the disease, recover quickly, and become firewalls—remain as potential carriers.
However, social distancing can keep hospitalizations at reasonable levels so that victims receive proper care, and it can also buy time to discover and mass-produce effective treatments. This is a distinct possibility in the short term, for as Michael Farzan, co‐chair of the Department of Immunology and Microbiology at Scripps Research, has stated, the same physical feature of the virus that makes it so contagious also makes it:
very vulnerable to antibody neutralization, and thus it is a relatively easy virus to protect against. I refer to it as “stupid” on a spectrum where HIV, which lives in the face of an active immune system for years, is a “genius.”
President Trump has touted a small French study showing that treatment with a combination of two drugs, hydroxychloroquine and azithromycin, “is significantly associated with viral load reduction/disappearance in COVID-19 patients….” The study was published in the International Journal of Antimicrobial Agents, and the 18 scholars who authored it wrote that the “results are promising” and “we recommend that Covid-19 patients be treated with” these drugs “to cure their infection and to limit the transmission of the virus to other people.” Nonetheless, media outlets have covered this matter by reporting that Trump “is not a doctor” and that he shouldn’t hype “unproven” and “untested” treatments or give people “false hope.”
Theatrics aside, the FDA has issued an Emergency Use Authorization that allows doctors to treat certain hospitalized Covid-19 patients with hydroxychloroquine and chloroquine “when a clinical trial is not available or feasible.” The authors of the French study make clear that their “study has some limitations including a small sample size, limited long-term outcome follow-up, and dropout of six patients from the study, however in the current context, we believe that our results should be shared with the scientific community.”
During a March 14th press conference, U.S. Surgeon General Jerome Adams asserted that “this situation will last longer, and more people will be hurt” if “we are complacent, selfish, uninformed,” and if “we spread fear, distrust, and misinformation.” Conversely, he said that “we will overcome this situation” if we “pitch in” and “share the facts.”
The vital facts above confirm the wisdom of his words.