Regulators at the European Union are warning that COVID-19 booster shots could compromise the immune system. The European Medicines Agency (EMA) stated that taking a booster shot every four months, as some have recommended, could weaken the immune system over time and adversely affect the body’s ability to ward off sickness.
“[Boosters] can be done once, or maybe twice, but it’s not something that we can think should be repeated constantly,” Marco Cavaleri, the EMA head of biological health threats and vaccines strategy, said. “We need to think about how we can transition from the current pandemic setting to a more endemic setting.”
Meanwhile, Pfizer is planning to release a new vaccine to target omicron. The United Kingdom Health Security Agency found that Moderna and Pfizer vaccinations were only 10% effective at preventing omicron after the second dose. Yet, countries like Israel have already begun administering a fourth shot to healthcare workers and people over 60. It started with a two-dose vaccine, then a booster. When does it end?
A few people have questioned my comment on Virginia Giuffre saying she was a victim of sex trafficking. I totally disagree. Just watch the movie Taken which is based on the real sex trafficking trade. There they kidnap girls who are then forced to have sex. That by no means applies to what Epstein was doing. He enticed girls into a high-level standard of living and they were trained how to have sex. They voluntarily joined that lifestyle which is substantially different from the girls who are really victims of the sex trade. I do not think it is appropriate to lump them all together into one group. The sex trade is a serious issue. I have always advised even our staff never to walk alone in the major cities of London, Paris, or Rome. They even have been kidnapping them in New York City. With this defunding of the police, it will only get worse. This is also unfolding in California.
Posted originally on the conservative tree house on January 15, 2022 | sundance | 41 Comments
In 1992, Suparna Dutta arrived in the US from India.
In 2020, Mrs. Dutta spoke to the Fairfax County VA school board. They ignored her.
In 2021, Suprana Dutta stood up, took a stand and worked to help Glenn Youngkin win the race for Virginia governor. Today, 2022, thirty years after arriving at the place of hope and opportunity for her family, she speaks at the inauguration of Governor Youngkin.
At the end of her inspiring *remarks Mrs. Dutta proclaims, “God bless the United States of America!”
Posted originally on the conservative tree house on January 15, 2022 | sundance | 187 Comments
Comrades, when we permit the government to gather private cell phone data, the government will always gather private cell phone data. In Canada the health officials have now admitted they captured, without legislative authority, the personal cell phone data and geolocation data of 33 million Canadians.
As a result, and a little late all things considered, privacy issues are being raised about the Public Health Agency of Canada (PHAC) buying the location data of Canadian cellphone users to monitor their activity. The agency said it wanted to analyze the movement of people during the pandemic to ensure their safety and well-being.
However, the implications of a totalitarian administrative state monitoring citizens under the guise of pandemic authority, does not make everyone feel comfy. John Brassard, a conservative member of parliament, questions the pandemic surveillance and legal authority. WATCH:
They are only secretly monitoring you for your health comrades, promise.
Byram W. Bridle, PhD, MSc, Associate Professor of Viral Immunology, Department of Pathobiology, University of Guelph, Guelph, ON, Canada, bbridle@uoguelph.ca
Bonnie A. Mallard, PhD, Professor of Immunogenetics, University of Guelph, Guelph, ON, Canada, bmallard@uoguelph.caSubscribe to the Trialsitenews “COVID-19” ChannelNo spam – we promise
Niel A. Karrow, PhD, MSc, Associate Professor, Department of Animal Biosciences, University of Guelph, Guelph, ON, Canada, nkarrow@uoguelph.ca
David J. Speicher, PhD, MSc, Senior Research Associate, Department of Pathobiology, University of Guelph, Guelph, ON, Canada, research@davidspeicher.com
Claudia Chaufan, MD, PhD, Associate Professor of Health Policy and Global Health, York University, Toronto, ON, Canada, claudia.chaufan@protonmail.com
Julian G.B. Northey, PhD, MSc, Adjunct Professor, Ontario Tech. University, Oshawa, ON, Canada, julian.northey@utoronto.ca
Steven Pelech, PhD, Professor, Department of Medicine, University of British Columbia, Vancouver, BC, Canada, spelech@mail.ubc.ca
Christopher A. Shaw, PhD, Professor, Department of Ophthalmology and Visual Sciences, University of British Columbia, Vancouver, BC, Canada, cashawlab@gmail.com
Ondrej Halgas, PhD, MSc, Biomedical Researcher, University of Toronto, Toronto, ON, Canada, ondrej.halgas@mail.utoronto.ca
Deanna McLeod, HBSc, Principal and Lead, Kaleidoscope Strategic, deanna@kstrategic.com
Citation: Bridle BW, Martins I, Mallard BA, Karrow NA, Speicher DJ, Chaufan C, Northey, JGB, Pelech S, Shaw CA, Halgas O, McLeod D. Concerns regarding the efficacy and safety for BNT162b2 mRNA coronavirus disease (COVID-19) vaccine through six months. http://www.CanadianCovidCareAlliance.org (January 10, 2022) 1-10.
Summary of concerns
Efficacy
• Important limitations of the stated efficacy claims were not discussed
• Only the relative risk reductions were stated; absolute risk reduction metrics were not presented
• Integration of adult and adolescent cohorts with differing follow-up periods were presented without explanation
• Large number of discontinued or missing participants comparable to primary end-point event numbers
• Prior SARS-CoV-2 infections screened only in a subset of trial participants, and determined only by an antibody test with severe sensitivity limitations
• Cut-offs of the RT-PCR positivity tests were not reported; no confirmatory functional virology assays were performed
• Absence of systematic testing and unbiased testing framework for the detection of SARS-CoV-2-infected participants
Safety
• Trial participants were healthier than the average population
• Monitoring of adverse events were limited in time and scope
• Number of severe adverse events in the vaccine arm were much higher than the numerical reduction in severe COVID-19 cases between vaccine and placebo arms
• Superficial evaluation of the most clinically relevant end-point – survival; no independent assessment of the causes of death provided
• Cardiovascular adverse vaccine events are now widely recognized, yet no systematic monitoring of cardiovascular health was carried out
• Substantially higher number of solicited and unsolicited adverse events, most of which presented as COVID-19-like symptoms, in the vaccine arm yet study claims efficacy against symptomatic COVID-19
• Increase in cardiac-related deaths in the vaccine arm compared to placebo arm
• Inability to assess long term safety within the trial due to unblinding and participant crossover to the vaccine arm
Other concerns
• Multiple conflicts of interest of a large majority of study authors
• Multiple trial irregularities reported by Thacker et al. (1) published in the British Medical Journal
Article
We present several concerns regarding the recent article by Thomas et al. (2) on the efficacy and safety of the BNT162b2 mRNA coronavirus disease (COVID-19) vaccine, which was published in the New England Journal of Medicine (NEJM) on November 4, 2021. An abbreviated version of this letter was submitted to the NEJM on November 15, 2021 and declined for publication on November 29, 2021 due to limited space. The study assessed the BNT162b2 in individuals that were healthy or had stable chronic medical conditions and concluded that, “through 6 month follow up, despite a gradual decline in vaccine efficacy, BNT162b2 had a favorable safety profile and was highly efficacious at preventing COVID-19.” We present numerous concerns regarding the reported safety and efficacy of this injection.
Efficacy
First, Thomas et al. (2) reported BNT162b2 efficacy as a relative risk reduction of contracting symptomatic reverse-transcriptase-polymerase chain reaction (PCR)-confirmed COVID-19 of 91.3% (77 vs 850 cases) and severe symptomatic PCR-confirmed COVID-19 of 96.7% (1 vs 30 severe cases). Thomas et al. (2) should have reported efficacy as an absolute risk reduction as per the communicating risks and benefits guidelines issued by the United States Food and Drug Administration (FDA) (3), which would have highlighted the modest absolute risk reductions provided by the vaccine in both symptomatic (3.7%) and severe symptomatic (0.7%) PCR-confirmed COVID-19.
Second, this analysis is the only published account of the BNT162b2 phase I – III trial efficacy outcomes among adults ≥16 years of age through six-month follow-up after immunization. In a trial amendment, a cohort of adolescents aged 12 to 15 years was added to the phase III study for which there was a shorter follow-up period. In this analysis, Thomas et al. (2) combined the two cohorts in providing efficacy outcomes after a six month follow up and departed from the initial analysis without providing a reasonable explanation for doing so. Given that vaccine efficacy wanes over time, by combining the older and younger cohorts, Thomas et al. (2) obfuscated the efficacy of the older group at six months. The authors should have provided efficacy outcomes for both groups and explicitly state the two reporting time periods in their conclusion.
Third, when discussing their findings, Thomas et al. (2) did not mention that a larger proportion of participants in the placebo group discontinued the trial compared to the vaccine group; 40% more after the first dose (271 vs 380 participants) and 63% more after the second dose (167 vs 273 participants). Discontinuations consisted mostly of “voluntary withdrawals”, “no longer meeting the eligibility criteria” and “lost to follow-up.” Additionally, there were a high number of participants missing from the CONSORT diagram between 2nd dose and the open-label period with more participants missing in the vaccine arm (1,258 vs 583 missing). These imbalances, which were in the order of the number of primary end-point events (77 and 850, for vaccine and placebo, respectively) call into question the reliability of these findings. Thomas et al. (2) should have disclosed the details related to the nature of these losses and discussed the impact they may have had on overall findings.
Fourth, Thomas et al. (2) used inappropriate tests when assessing current or prior infections due to severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2). The authors screened 10,453 serum samples for COVID-19 infections up to 6 weeks prior to enrollment using the Roche Elecsys® Anti-SARS-CoV-2 antibody test, which tests for only the nucleocapsid protein of SARS-CoV-2 and has high sensitivity 14 days after infection when antibodies tend to peak (4). However, as antibody levels wane over time despite persisting immunity, it is unlikely that this test alone could identify prior immunity to SARS-CoV-2 or distinguish between prior immunity to other coronaviruses, which express similar proteins. Additionally, testing for the SARS-CoV-2 was done with the Cepheid Xpert Xpress SARS-CoV-2 RT-PCR rather than the gold-standard functional virology assay, looking for cytopathic effect in permissive cells. FDA specifications for PCR testing at that time the trial was conducted tended toward cycle thresholds beyond 20-30 cycles (5), which are now widely recognized as being unreliable in detecting an active COVID-19 infection (6-8). Given these limitations, Thomas et al. (2) should have used better screening for natural immunity, used a functional virology assay, and discussed the implications of these testing limitations in their findings.
Fifth, we noted an absence of systematic testing and an objective testing framework for the detection of SARS-CoV-2-infected participants. In this study, it was left to the discretion of the investigator to send a patient presenting with COVID-19-like symptoms for laboratory confirmation of SARS-CoV-2 infection, a task which would be particularly difficult given that reactogenicity events consisted principally of COVID-19-like symptoms (Thomas et al. (2), Figure S1). This lack of systematic testing introduced a concerning level of variability and subjectivity associated with the identification of both symptomatic cases and disease severity (9,10). Thomas et al. (2) should have discussed the implications of this lack of objective and systematic virological assessment on their study findings as well as presented data related to asymptomatic testing that was conducted at “selected sites.” Overall, the emphasis on relative risk reductions, the combining efficacy outcomes from the adult and adolescent cohorts, the large number of people who were excluded from the analysis, and the use of inappropriate tests and lack of objective testing framework call into question the authors’ conclusions regarding vaccine efficacy.
Safety
First, Thomas et al. (2) concluded their article by stating that BNT162b2 showed a “favorable safety profile,” and in their abstract stated that “BNT162b2 continued to be safe and have an acceptable adverse-event profile.” However, Thomas et al. (2) Figure S1 summarized solicited adverse events reported within 7 days of the first dose in the reactogenicity subset, which represented a mere 22% of the randomized population. A considerably higher rate of local and systemic adverse events was reported among vaccine recipients with a marked increase in adverse events with the second dose. The preponderance of systemic effects in both arms were COVID-19-like symptoms and occurred at higher rates than in the vaccine compared to the placebo group, despite the vaccine group having a higher number of identified symptomatic COVID-19 cases (77 vs 850, vaccine vs placebo, respectively). The very need for this trial is predicated on the importance and clinical relevance of eradicating COVID-19 symptoms. How is it then that such consistent increases in COVID-19-like symptoms among vaccine recipients are described as “favorable”?
Second, Thomas et al. (2) provided a descriptive analysis of vaccine safety. To better compare the benefits and the risks of this vaccine, we calculated absolute and relative risk reductions/increases (ARR/ARI and RRR/RRI, respectively) associated with the vaccine for efficacy events seven days after the second dose (i.e., corresponding to full vaccination for those in the vaccine group) and for safety events during the respective data collection period (starting with the first-dose). These calculations were based on the eligible population for each relevant safety and efficacy events without adjusting for surveillance time as that data was not published for safety events. A simple chi-square calculator was used to assess the significance of the difference in event numbers between groups (Table 1) (11).
Table 1. Differences in the number of efficacy and safety events in eligible populations¥ reported in the 6-month update of the BNT162b2 mRNA Covid-19 vaccine
Event
BNT162b2(n)
Placebo(n)
Absolute Difference (p-value)?
Absolute Risk Change* (%)
Relative Risk Change* (%)
Cases Adults and Adolescents 7 days after 2nd dose$
77
850
-773 (p<0.00001)
-3.7
-90.9
Any Unsolicited Treatment-Related Adverse Event Adults#
5,241
1,311
+3,930 (p<0.00001)
+17.9
+299.7
Any Severe Event Adults/
390
289
+101 (p=0.0001)
+0.5
+34.9
Severe Cases in Adults 7 days after 2nd dose&
1
23
-22 (p<0.00001)
-0.1
-95.7
Unsolicited Severe Adverse Events~ AdultsPrevents daily routine activity or requires intervention or worse
262
150
+112 (p<0.00001)
+0.5
+74.6
Serious Adverse Event Adults§Requires hospitalization or results in permanent injury or death
127
116
+11(p=0.5)
+0.05
+9.5
Deaths during placebo-controlled period [additional deaths during open-label period in vaccine recipients or placebo-only]%
15 [+5]
14 [NR]
+1 [+5](p=0.9)
+0.005
+7.1
Deaths due to cardiovascular events^
9
5
+4
¥ For the purpose of this table and in accordance with the terminology used in the study report, adult and adolescent populations are defined as ≥16 years old and 12-15 years old, respectively.
? Significance figures (p-values) estimated using chi-square calculator available at https://www.socscistatistics.com/tests/chisquare. P-values are without the Yates correction. This procedure was applied following the framework used by Classen (11) in his analysis of “All Cause Severe Morbidity” based on data from the initial reports of the vaccine Phase III trials
* Authors estimated vaccine efficacy using total surveillance time as denominator, however, as this value was unavailable for all the events analyzed, our calculations used the common statistical definition, i.e., number of events relative to total number of eligible patients for each event analysis reported29 similar to previous analyses of this nature (11-30);
$ ≥7 Days after dose 2 among participants without evidence of previous infection
# Adverse events reported outside of the reactogenicity subgroup and assessed by the investigator as related to investigational product
/ In calculations combining efficacy and safety events, the number of patients randomized that received any dose of vaccine or placebo was used as the study population in the statistical calculations, following the framework used by Classen (11) in his analysis of “All Cause Severe Morbidity”. Differences in the total (event-incident) population (randomized vs efficacy vs safety) used as denominator are relatively small and are expected to have minimal impact on the relative differences between groups. Without access to individual patient data, these calculations were performed under the assumption that efficacy and safety events were non-overlapping
& ≥7 Days after dose 2; confirmed severe COVID-19 defined as PCR-positivity and “presence of at least one of the following: • Clinical signs at rest indicative of severe systemic illness (RR ≥30 breaths per minute, HR ≥125 beats per minute, SpO2 ≤93% on room air at sea level, or PaO2/FiO2 <300 mm Hg); • Respiratory failure (defined as needing high-flow oxygen, noninvasive ventilation, mechanical ventilation, or ECMO); • Evidence of shock (SBP <90 mm Hg, DBP <60 mm Hg, or requiring vasopressors); • Significant acute renal, hepatic, or neurologic dysfunction;• Admission to an ICU; • Death”
~ Severe (grade ≥3) adverse events were generally defined as those that interfere significantly with participant’s usual function, those that affect daily living or require medical care; grade 4 events were generally defined as those that required emergency room visit or hospitalization
§Serious adverse events were defined as any untoward medical occurrence that, at any dose: a. Results in death; b. Is life-threatening; c. Requires inpatient hospitalization or prolongation of existing hospitalization; d. Results in persistent disability/incapacity.
% Deaths during the open-label period were reported only in vaccine recipients, 3 participants in the BNT162b2 group and 2 in the original placebo group who received BNT162b2 after unblinding
^Those with reported cause of death due to: aortic rupture, arteriosclerosis, cardiac arrest, cardiac failure congestive, cardiorespiratory arrest, hypertensive heart disease, or myocardial infarction
Our findings showed that the increase in unsolicited adverse events in vaccine recipients, which included at least one adverse event up to 1 month post the second dose, was greater (RRI of 299.7% and ARI of 17.9%; p<0.00001) than the reduction in identified symptomatic COVID-19 cases observed in fully-vaccinated individuals for the duration of the trial (RRR of 90.9% and ARR of 3.7%; p<0.00001).
A similar pattern was observed for severe and serious adverse events. The study concluded that “vaccine efficacy against severe disease was 96.7%.” However, our analysis showed that the vaccine was associated with a significant increase in severe adverse events defined as an adverse event that interferes significantly with daily activity or requires medical care (RRI of 74.6% and ARI of 0.5%; p<0.00001) and a numerical increase in serious adverse events, defined as any untoward medical occurrence that was life-threatening, required hospitalization or resulted in persistent disability up to 6 months (RRI of 9.5% and ARI of 0.05%; p=0.5) compared to placebo. These increases were greater than the reduction in severe COVID-19 cases observed in fully-vaccinated individuals for the duration of the trial (RRR of 95.7% and ARR of 0.1%; p=0.00002). When severe COVID-19 events were pooled with severe or serious adverse events to determine the likelihood of experiencing any severe event (11), there was an overall increase in severe events among vaccine recipients compared with placebo (RRI of 34.9% and ARI of 0.5%, p=0.0001). Given these findings, Thomas et al. (2) should have revised their conclusion to state, “the vaccine was associated with a concerning and clinically meaningful increase in severe events relative to placebo.”
Third, Thomas et al. (2) conducted minimal monitoring of adverse events (12). Firstly, the solicited reactogenicity data was collected for only a small portion of trial participants (9,839/44,047 or 22.3%), for a limited 7 days after each dose, and for only a short pre-specified list of systemic and injection site reactions with no monitoring of sub-clinical effects. Secondly, unsolicited adverse events were collected for a mere 1 month and serious adverse events for only 6 months following the second dose. This means that severe vaccine related cardiac, neurological or immunological injuries that took more than a month to diagnose and were not considered serious, would not be reflected in the findings. Thirdly, unblinding and subsequent crossover of those on the placebo arm to the vaccine arm, will certainly attenuate any safety signals coming from this trial as well as preclude insights into long-term safety which were to be monitored for 2 years. Thomas et al. (2) should have commented on the implications their abbreviated monitoring schedule may have on safety underreporting as well as the implications of unblinding on short- and long-term safety outcomes. Given the increase in severe events (RRI of 34.9% and ARI of 0.5%) and cardiovascular deaths associated with the vaccine (n= 9 vs 5, vaccine vs placebo, respectively), The authors should have more closely monitored safety and provided a detailed discussion of the severe and serious adverse events along with a discussion of their potential long-term implications.
Fourth, given the inclusion of adolescents and “healthy participants who had stable chronic medical conditions” in the study population, we noted very little discussion of death, the most clinically relevant end-point of this trial. Thomas et al. (2) Table S3 showed a slightly higher number of deaths in the vaccine group (n=15 vs n=14 in the placebo group during the blinded period). However, the manuscript text (Thomas et al. (2), page 7) stated that five additional deaths occurred in vaccine recipients after unblinding (two of which were initially allocated to the placebo group) for a total of 20 deaths in vaccine recipients. Thomas et al. (2) Table S4 also showed that although only 3 study deaths were attributed to COVID-19 or COVID-19 pneumonia (n=1 vs n=2, vaccine vs placebo, respectively) a total of 14 deaths were cardiovascular in nature (aortic rupture, arteriosclerosis, cardiac arrest, cardiac failure congestive, cardiorespiratory arrest, hypertensive heart disease) with the almost twice as many occurring in the vaccine arm (n=9 vs n=5, vaccine vs placebo, respectively). There is currently an abundance of real-world evidence to support an association between cardiovascular adverse events and the vaccines (13-17). Thomas et al. (2) reported that “none of these deaths were considered to be related to BNT162b2 by the investigators” without describing the objective framework of testing that allowed them to arrive at that conclusion or whether their findings were independently evaluated. Given the seriousness of these adverse events in an otherwise healthy population, Thomas et al. (2) should have provided a detailed description of how they arrived at their conclusion, these evaluations should have undergone independent assessment, and all ongoing study protocols investigating BNT162b2 should be immediately amended to include systematic short- and long-term clinical and sub-clinical monitoring of cardiovascular health. Overall, the increased rates of COVID-like symptoms, unsolicited adverse events as well as severe and serious adverse events in the vaccine compared to the placebo arm, as well as the net increase in deaths in vaccine recipients compared with those who were unvaccinated present serious concerns regarding the safety of these biological agents.
Conflicts of Interest
The disconnect between author conclusions, our analysis of the data, and the NEJM rejection of our letter to the editor led us to examine author disclosures for potential conflicts of interest (COI) (Table 2). Our analysis revealed multiple direct conflicts of interest. The article was supported by BioNTech and Pfizer, the corresponding author, Judith Absolon, and the senior author, Kathrin Jansen were employees of Pfizer and owned company stock, and the first author Stephen Thomas was a consultant to Pfizer. Of the 32 authors, 21 (66%) were employees of Pfizer or BioNtech and 26 (81%) had Pfizer/BioNtech-related conflict of interests. We also noted that one of NEJM’s senior editors is also a co-principal investigator of the related Moderna-Vaccine COVE-trial (18,19).
Table 2. Conflicts of interest related to Pfizer/BioNTech
Title
Author
Corresponding author
Judith Absalon: Pfizer employment and stock holder
First author
Stephen Thomas: Pfizer consultancy
Last author
Kathrin Jansen: Pfizer employment and stock holder
Other 29 authors (66% employees, 81% had some COI)
Pfizer/ BioNTech employment and stockholder, n=15; Pfizer/ BioNTech employment (without stock) n=4; Pfizer grant/contract n=3; Pfizer clinical trial n=1; Other company consultancy n=1; No COI n=5
Conclusion
Our critique of the Thomas et al. (2) publication revealed multiple concerns regarding author claims of BNT162b2 safety and efficacy as well as a high number of direct conflicts of interest in the publication authors. These, coupled with multiple reports indicating that vaccine efficacy wanes within months of administration (20-23), reduced effectiveness of BNT162b2 with respect to emerging variants (24-26), record rates of serious adverse events (122,833) and deaths (17,128) reported in the US passive Vaccine Adverse Event Reporting System, VAERS by October 16, 2021, and problems with data integrity in the conduct of this trial reported recently by Thacker (1) in the British Medical Journal, raise further concerns regarding both the efficacy and safety of this agent. We did not find sufficient evidence to support use of these agents in the healthy adults studied or in specific unstudied demographics that are being mandated to comply with vaccination including the naturally immune, the frail elderly, those with multiple co-morbidities, the immunocompromised, and pregnant women. It also calls into question use in adolescents and children given that companion trials conducted in those populations suffered from similar design flaws, including underpowered in participant numbers and that recommendations for use were based on minimal safety follow up (27,28).
Conflicts of Interest
Byram W. Bridle received funding from the Ontario Government (COVID-19 Rapid Research Fund, Ministry of Colleges and Universities) and Government of Canada (Pandemic Response Challenge Program, National Research Council of Canada) to conduct pre-clinical research with COVID-19 vaccines
Ilidio Martins, none to disclose
Claudia Chaufan, none to disclose
Julian Northey, none to disclose
Niel A. Karrow, none to disclose
Steven Pelech is the majority shareholder and president and Chief Scientific Officer of Kinexus Bioinformatics Corporation, which has been developing serological tests for detection of antibodies against SARS-CoV-2 proteins and testing of drugs to inhibit SARS-CoV-2 replication
Bonnie Mallard, none to disclose
Christopher A. Shaw has been an expert witness in Vaccine Court twice
David Speicher, none to disclose
Ondrej Halgas, none to disclose
Deanna McLeod, none to disclose
References
1. Thacker PD. COVID-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial. BMJ 2021;375:n2635.
2. Thomas SJ, Moreira ED, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine through 6 months. N Engl J Med 2021;385:1761-73.
3. Fischhoff B. Communicating risks and benefits: An evidence based user’s guide. Silver Spring, MA, USA: Food and Drug Administration (FDA), US Department of Health and Human Services. Government Printing Office; 2012.
5. Cepheid. Xpert® Xpress SARS-CoV-2 – Instructions for use. For use under an Emergency Use Authorization (EUA) only. U. S. Food and Drug Administration, 2021. (Accessed June 29, 2021, at https://www.fda.gov/media/136314/download.)
6. Mina MJ, Peto TE, García-Fiñana M, Semple MG, Buchan IE. Clarifying the evidence on SARS-CoV-2 antigen rapid tests in public health responses to COVID-19. The Lancet 2021;397:1425-7.
7. Al Bayat S, Mundodan J, Hasnain S, et al. Can the cycle threshold (Ct) value of RT-PCR test for SARS CoV2 predict infectivity among close contacts? Journal of Infection and Public Health 2021;14:1201-5.
11. Classen B. US COVID-19 vaccines proven to cause more harm than good based on pivotal clinical trial data analyzed using the proper scientific endpoint,“All cause severe morbidity”. Trends Int Med 2021;1:1-6.
13. Rose J. A Report on the US Vaccine Adverse Events Reporting System (VAERS) of the COVID-19 messenger ribonucleic acid (mRNA) biologicals. Sci, Pub Health Pol, & Law 2021;2:59-80.
14. Kaur RJ, Dutta S, Charan J, et al. Cardiovascular adverse events reported from COVID-19 vaccines: A study based on WHO database. Int J Gen Med 2021;14:3909.
15. Aye YN, Mai AS, Zhang A, et al. Acute myocardial infarction and myocarditis following COVID-19 vaccination. QJM: monthly journal of the Association of Physicians 2021.
16. Diaz GA, Parsons GT, Gering SK, Meier AR, Hutchinson IV, Robicsek A. Myocarditis and pericarditis after vaccination for COVID-19. JAMA 2021;326:1210-2.
17. Barda N, Dagan N, Ben-Shlomo Y, et al. Safety of the BNT162b2 mRNA COVID-19 vaccine in a nationwide setting. N Engl J Med 2021;385:1078-90.
18. Baden LR, El Sahly HM, Essink B, et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med 2021;384:403-16.
19. Keil U. Re: COVID-19: How independent were the US and British vaccine advisory committees? BMJ 2021;373:n1283. 2021. (Accessed Dec 6, 2021, at Re: COVID-19: How independent were the US and British vaccine advisory committees?)
20. Goldberg Y, Mandel M, Bar-On YM, et al. Waning immunity after the BNT162b2 vaccine in Israel. N Engl J Med 2021.
21. Puranik A, Lenehan PJ, O’Horo JC, et al. Durability analysis of the highly effective BNT162b2 vaccine against COVID-19. medRxiv 2021.
22. McDade TW, Demonbreun AR, Sancilio A, Mustanski B, D’Aquila RT, McNally EM. Durability of antibody response to vaccination and surrogate neutralization of emerging variants based on SARS-CoV-2 exposure history. Sci Rep 2021;11:1-6.
23. Andrews N, Tessier E, Stowe J, et al. Vaccine effectiveness and duration of protection of Comirnaty, Vaxzevria and Spikevax against mild and severe COVID-19 in the UK. medRxiv 2021.
24. Collie S, Champion J, Moultrie H, Bekker L-G, Gray G. Effectiveness of BNT162b2 vaccine against Omicron variant in South Africa. N Engl J Med 2021.
25. Lefèvre B, Tondeur L, Madec Y, et al. Beta SARS-CoV-2 variant and BNT162b2 vaccine effectiveness in long-term care facilities in France. The Lancet Healthy Longevity 2021;2:e685-e7.
26. Hansen CH, Schelde AB, Moustsen-Helm IR, et al. Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study. medRxiv 2021:2021.12.20.21267966.
27. Frenck RW, Jr., Klein NP, Kitchin N, et al. Safety, immunogenicity, and efficacy of the BNT162b2 COVID-19 vaccine in adolescents. N Engl J Med 2021;385:239-50.
28. Walter EB, Talaat KR, Sabharwal C, et al. Evaluation of the BNT162b2 COVID-19 vaccine in children 5 to 11 years of age. N Engl J Med 2021.
Posted originally on the conservative tree house on January 15, 2022 | Sundance | 58 Comments
In the Netherlands the typically high-brow, polite and social society has been a little shocked at how the Dutch proles have begun to express anger toward the totalitarian dictates of the professional political class.
Amid this class-driven über-sensitive social fabric, Dutch Prime Minister Mark Rutte is now in the tenuous position of holding a governmental system together with a coalition of disparate leftist groups who are, well, a little eclectic all things considered.
As noted recently “One of the biggest challenges for the new government is the rise in public mistrust and anger towards politics and politicians. The Netherlands has seen some of Europe’s biggest opposition and protests against government COVID-19 policy. Many Dutch lawmakers say they don’t feel safe. Some of them now have to be protected by police around the clock – a shock in a country where ministers often ride bicycles rather than use their official cars.” (link)
The land of skinny pant beta males has, as the most sensitive progressives would expect, put women into all of the systems of government to showcase their civic investment and high-minded multicultural progress. The Netherlands is the type of place where Davos attendees feel comfy sipping filtered dew from the petals of spring tulips and discussing the best way to save the planet from the scourge of the shallow working class. Okay, so that’s the context…
Into this mix comes a young Dutch wolverine, a new Member of Parliament named Gideon van Meijeren; who appears to be a rather cheeky rebel, quite comfortable telling the elite they look silly. THIS you have to watch to appreciate (Direct Rumble Link):
Posted originally on the conservative tree house on January 14, 2022 | Sundance | 456 Comments
The Australian Open is scheduled to begin January 17th in Melbourne, the epicenter of Australia’s totalitarian COVID mandates. Australia granted unvaccinated tennis superstar Novak Djokovic a visa to compete. Australian border officials then attempted to block his entry and deport him because he was unvaccinated.
Novak Djokovic took the issue to the federal court in Australia and won his legal case against the Australian government. However, earlier today Australian Immigration Minister Alex Hawke unilaterally cancelled his visa.
Under Australian law, Immigration Minister Hawke has almost unfettered powers to cancel a visa making any legal challenge to the decision very difficult. The official statement from Alex Hawke is AVAILABLE HERE.
Today I exercised my power under section 133C(3) of the Migration Act to cancel the visa held by Mr Novak Djokovic on health and good order grounds, on the basis that it was in the public interest to do so. This decision followed orders by the Federal Circuit and Family Court on 10 January 2022, quashing a prior cancellation decision on procedural fairness grounds.
In making this decision, I carefully considered information provided to me by the Department of Home Affairs, the Australian Border Force and Mr Djokovic. The Morrison Government is firmly committed to protecting Australia’s borders, particularly in relation to the COVID-19 pandemic. (read more)
Sky News has the following article: […] Following a federal court’s decision to overturn the original decision to cancel Djokovic’s visa, the government indicated it would consider using ministerial discretion to deport the Serbian tennis star.
Following days of delay, Mr Hawke finally announced his decision under Migration Act which gives the minister full discretion to deport a person. Mr Hawke said the cancellation of Djokovic’s visa was made on the grounds of “health and good order” as well as on the basis of the “public interest”. (read more)
Note that views expressed in this opinion article are the writer’s personal views and not necessarily those of TrialSite.
By Omar Kahn
Before diving into our decalogue, a little brush clearing is in order.
“Mainstream media” is now largely owned by clearly vested interests, influenced by advertising (overwhelmingly so by industry) and is far from a “public trust” in the sense it might have been perceived so in the past. Grant money intimidates “scientists.” And sponsors, advertisers and others govern what we might hear and see and perhaps therefore “think.” Subscribe to the Trialsitenews “COVID-19” ChannelNo spam – we promise
“Science” in terms of genuine research and the exploring, challenging, and expanding of hypotheses using evidence and replicable testing is far apart from “scientific conclusions” being touted in mainstream or even so called “academic” media primarily for behavioral and psychological influencing.
The “science” politicians follow is the latter. And ambiguity is the enemy. Take “germ theory”, a hardy, apolitical postulate. If we mean “capable of causing disease” many mostly safe microbes get entered into the inventory. The list of those that always cause disease and are never harmless reduces us to a list of painfully few if any. This is the grand larceny at the heart of the PCR fiasco, where “presence” of microbes is broadcast, not actual “infection” which would be accompanied by symptoms.
So, the template we’ve been inundated with via media channels is more “magical” contagion, stoking hysteria, inflicting pointless measures that meaninglessly choke the human spirit. The UK modeling body SAGE (of Imperial College modeling shame), confessed via the Chair of their committee, Graham Medley in early December that they are explicitly ordered to produce worst case scenarios to enable political leverage. If accuracy was a key performance indicator, these eminent modelers would have been ceremoniously sacked, they might have been sued for outright fraud. And if applying the negligence criteria of US Tort Law, one shivers to think how to assess the ripple effects and catastrophic collateral damage.
We have a parody of “analysis”, incompetence coupling with arrogance, the laundering of data to justify decisions, dealing with people’s lives with a detached mania that beggars description. The role of media should have been akin to H.L. Mencken’s description of what his role was, “To comfort the afflicted and afflict the comfortable.” Instead, they perfected their servility and their PR skills.
Not Novel
The word ‘novel’ insofar as it relates to viruses would literally mean no pre-existing cross reactive partial immunity. So, the diseases that accompanied Columbus to the Americas killed up to 95% of North and South America’s indigenous population. That is what real ‘novelty’ does.
Today when “novel” was affixed to COVID, contextually scientists knew that referred to a newly emergent strain. The general public by contrast was invited to jump to the conclusion that this was an entirely new virus as when TB or influenza went to the Americas. Scientists stayed unforgivably mum and brandished novelty in a slapdash fashion.
This corrosive bit of wordsmanship, augmented by propaganda, innuendo, terrifying visual icons, produced a wave of fear so strong that people were irrationally lusting for a leaky jab to make them “safe” and were willing to coerce friends, neighbors and family members to similar extremes. Countries like Canada, to our chagrin, have actually made acting on such incoherent misunderstanding mandatory.
Back when we were being terrified by the collapsing Wuhanese on our TV screens, the Diamond Princess cruise ship sailed into view offering sanity and far greater serenity, had we only partaken of its lessons.
The virus circulated freely on board what was essentially, inadvertently, a floating petri dish, and produced age corrected lethality of merely 0.025% to 0.625% (that’s a bad flu season). The Spanish Flu ranged between 2% and 10%. Only 26% of the passengers tested positive and despite being elderly 48% of those remained symptom free.
So, the Diamond Princess was not a floating morgue from bygone eras as it would’ve been if any of our assumptions and the Chinese graphics had been at all accurate. The only plausible explanation for that lack of deadliness is most people already having sufficient cross-reactive immunity from other coronaviruses or related pathogens.
This data was publicly available by February 2020. How, in the face of that, we launched “operation warp speed” to develop vaccines at the end of April 2020 eludes rationality. So, our health authorities knowingly, opportunistically and cynically imposed lockdowns, lobbied to suspend life until we had vaccines, though it was clear from this and other examples that were soon evident (seroprevalence studies from Dr. Ioannidis of Stanford, for example), no apocalypse was forthcoming, and we primarily needed to avail of early treatment and to shield the vulnerable.
Not Equally Lethal
Despite the charade of suggesting ‘no one is safe,’ there are vast differences between different demographics in terms of risk. It is a highly discriminatory virus, in fact. The people over 75 are an astonishing 10,000 times more at risk than those under 15, says Professor Mark Woolhouse, an expert on infectious diseases at Edinburgh University. The median age of death globally has been 82. The ‘pandemic’ (called that only because of verbal sleight-of-mind by the WHO in changing the definition away from lethality to simply rising cases), tracks normal mortality (average COVID age of death is higher than life expectancy) and so was materially different in terms of quality-of-life years affected compared to virtually any pandemic on record, especially from the Spanish Flu onwards, where the young were primary victims and clearly at heightened risk.
Not only has there been no sustained global excess mortality from 2020 on, many regions have had record lows in terms of mortality, parts of Africa and Asia among them, Sweden has had negative net mortality for the last two years in aggregate. Below the age of 70 without multiple chronic illnesses, there remains over a 99% chance of recovery.
Children are at virtually no risk at all. As demonstrated by Sweden where schools were kept open throughout, not only were there no deaths among the students, but transmissibility to teachers was virtually nil as well. It was one of the safest and ‘unmasked’ working environments in the world. The impact on the young is of recent vintage, post “vaccination”
From vs With
Death certificates proclaim a “COVID death” based on the mere presence of a positive test within 28 days of someone passing. Healthcare officials from the UK, Italy, Germany, and more are on record admitting to this practice. The US has even more egregiously said if C-19 “could have been the cause” there is discretion to tag the death as such, and insurance incentives for doing so. Dr. Ngozi Ezike confirmed in a press briefing in the US, that if you were in hospice with a few weeks to live, and “tested” COVID positive, you were listed as a COVID death. This flies in the face of any mortality accounting for any cause of death much less pandemic in historic memory, as none of those were pharma PR campaigns posing as public health.
Moreover, comorbidities galore compound this. Lombardy, after their hellish 2020 experience, published via their head of public health, statistics showing 99.2% of COVID deaths had at least one serious comorbidity, and only 12% could plausibly have been said to have, to some extent, died “of” COVID.
The pattern has held up around the world. The UK in October 2020 via the ONS reported less than 10% of the official death count ascribed to COVID, had it as the exclusive cause of death.
Lockdowns are Incoherent and Self-Destructive
Never in history have we locked up the healthy. In the Middle Ages, before spread extended (or so it was hypothesized), a village may have been “locked down” and food delivered there, until the pathogen could spread, become endemic and those afflicted would no longer be carriers. It was a penal solution, even there, and never replicated.
It was discouraged in every public health guideline through 2019, including WHO, US, UK, Europe and Australia. No new studies or evidence, much less randomized controlled trials, emerged to change the guidance. A few freakish, clearly contrived Wuhan videos, that seem laughably absurd today, were enough to overturn decades of medical research, guidance, evidence and wisdom…because it suited certain vested interests and power blocs.
Data has not been kind to this. First, virtually no transmission outdoors. Even the US CDC says, “less than 1%.” If so, why lock people in? Sunshine and fresh air are fatal to viruses, which is why the seasonality needle is what it is. Why deprive people of these? The two biggest comorbidities, as per the CDC, are obesity and anxiety. So we limit movement and channel 24/7 panic porn? Mindless and medically insane.
Unlocked down Japan, Florida since September 2020, Sweden throughout, have done no worse, and frankly much better in terms of all-cause mortality, age adjusted, than the lockdown havens, the US coasts, UK/France/Germany, etc.
There is in fact strong evidence lockdowns kill more than the “virus” (with a 99%+ recovery rate for virtually everyone remember). Dr. David Nabarro confessed world poverty will have doubled by 2022, child malnutrition will have doubled. He pegged it, “This is a terrible, ghastly global catastrophe.” And self-inflicted.
Unemployment, poverty, suicide, deaths from deferred treatments (surgeries and screenings) will all stockpile the negative impact of this misguided attempt to “lock in” an airborne virus, which is incoherent at its core as Professor Risch of Yale has highlighted. Wave after wave rolls in seasonally making a mockery of our fact-free hubris here.
PCR Tests Don’t “Diagnose”
These were never designed to diagnose illness. It amplifies what is there, and does not tell you if it’s a strand, a fragment, viral debris or “live” infectiousness. It also throws off reams of false positives, particularly at higher amplification settings, and though we know the Ct (Cycle Threshold) settings should be below 28, jurisdictions set them as high as 35 (or higher), and there is no global standard to this date!
This clearly shows we are not “diagnosing” we are simply “spinning” an illusion of runaway infectiousness with forebodings of lethality. And for the first time in medical history, we have redefined a “case” to be a “positive test” rather than the “presence of symptoms.” Even WHO has somewhat backpedaled on this, as it stretches credulity to a breaking point, but that “correction” is sequestered in the small print on their highly malleable website.
Chinese studies have shown the same patients can get two different results on the same day. The EUA of the original PCR test has been withdrawn now in the US, as they have finally admitted it cannot distinguish between influenza and COVID. These same tests precipitated an entirely fake whooping cough epidemic, reported on by The New York Times (back when it was still in the reporting business) in 2007.
A Portuguese court ruled PCR tests were unreliable and therefore inapplicable, the Swedes came to a similar conclusion. Way back in February 2020, the President of the Chinese Academy of Medical Sciences said “The accuracy of the tests is only 30-50%.” Oh yes, a perfect basis for blowing up and quarantining the world.
Though Germany’s Robert Koch Institute says, “nothing over 30 cycles is likely to be infectious” and the Harvard School of Public Health confesses that reducing these amplification settings from 40 (staggeringly commonplace in key US States) to 30, would have reduced “cases” in some States by as much as 90%, we still march on with no global benchmark enforced. How can “travel” be sanely synchronized without this being the case?
Asymptomatic Malarkey
As per our ‘non-test’ 75-85% of ‘COVID cases’ experience no viral symptoms at all. Ergo, how would you know the difference between the purportedly ‘asymptomatic’ and false positives? There is no clear clinical evidence of asymptomatic spread, though WHO had to tap dance politically for ‘leaking’ the truth.
Maria Van Kerkhove, head of WHO’s emerging diseases unit, way back in June 2020 said, “From the data we have it still seems to be rare that an asymptomatic individual actually transmits onward to a secondary individual.” A JAMA (Journal of the American Medical Association) meta-analysis found less than 1% chance of asymptomatic infection within a household and it was unclear that this was not ‘presymptomatic.’
A multimillion-person study in Wuhan failed to turn up even one credible corroborated instance. Two of the world’s leading COVID care practitioners with overwhelming success, Dr. Peter McCullough from the US and Dr. Shankara Chetty from South Africa, both say they have not seen one credible instance in the thousands upon thousands of patients they have treated.
Therefore, the simple remedy is to stop mass testing as we have no idea what the positive tests actually reveal if anything. We should therefore focus on the symptomatic as we have throughout medical history when not propagating a narrative for profit or other sundry motives. Life would go back to normal tomorrow. And without these misleading “cases”, no one would know anything unusual was virally or pathogenically afoot in the world.
It’s Highly Treatable
Little enough to say here other than what Dr. Tyson has highlighted, COVID is a consortium of symptoms, and all of the symptoms associated with the different phases of the illness (viral, inflammatory, thrombotic) have abundant, efficacious, safe, on and off label treatments that would normally, and should now be, at a doctor’s discretion.
Instead, shameful smear campaigns, fraudulent and later debunked ‘medical’ articles, complete disinterest in studying promising treatments, the inhumanity of the medical malpractice of telling doctors not to treat unless and if someone presents themselves at ICU, should, taken together, have been a megawatt medical scandal instead of being ‘rationalized’ by the sycophancy of the mainstream media. The overwhelming beneficial results produced globally through early treatment in reducing COVID-related mortality to virtually zero, where applied, is still begging to be broadcast.
Mask Stupidity
Dozens of scientific studies have shown that masks do nothing to stop the spread of respiratory viruses. The size of the nano particles almost mandates the conclusion despite desperate attempts to flog studies into serving up some pittance of credibility for this symbolic, totemic mass compliance exercise. The US CDC itself published a meta-analysis in May 2020 saying it found “no significant reduction in influenza reduction with the use of face masks.” In fact, going back, there is the damning (and never factually contradicted) 2015 study in the British Medical Journal (BMJ) showing that cloth masks were penetrated by 97% of particles and likely increase infection risk by retaining moisture as well as via the ubiquity of repeated use.
Globally, again, Sweden and Florida demonstrate, as does South Dakota compared to North Dakota, zero negative impact from the absence of mask mandates. In Kansas counties without mask mandates had fewer COVID ‘cases’ than counties with them. Breathing in your own waste, breathing in plastic microfibers which are said to be carcinogenic and getting insufficient oxygen, and the sheer lack of any rational benefit, are all reasons to push back zealously against this cult identity badge.
The ‘Vaccines’ that Weren’t
As an historical benchmark, pre-2020 no successful vaccine against a human coronavirus had ever been developed. Looked at soberly that record still stands. However, we are alleging that we somehow made 20 of them in 18 months!
Past attempts have created hyper sensitivity to the SARS virus which may be today why the booster race is on. These mRNA ‘vaccines’ which claim to reduce severity or likelihood of serious disease, but which do not stop reinfection or transmission and inject spike proteins (which is precisely what causes damage via COVID) are better described as therapeutics.
When we say the ‘vaccines’ do not confer immunity or ward off passing the disease onto others, BMJ highlights that the ‘vaccine’ studies were never even designed to assess this. The manufacturers themselves defined their products’ ‘efficacy’ as “reducing the severity of symptoms.”
Moreover, instead of years of safety trials which have been the irreducible minimum in terms of medical practice, these ‘vaccines’ were developed and approved in less than a year. They skipped early-stage trials altogether, and late-stage human trials have either not been peer reviewed or have not released their data. The overall safety trials will not even be done until 2023, and they have jabbed the placebo group since, so no control group is available, in a shocking departure from established practice. And, of course, these vaccinatory harlots have been granted legal indemnity.
And why is it not breaking news every day that under these conditions ‘informed consent’ as per the Nuremburg standard is completely unachievable and the push to inject these untested substances into children is nothing short of abominable?
The Truth is in Tatters
We have usually hoped that investigative journalists would be a wall of defense against illiberal and capricious propaganda fear induced by the state. But these barricades lie abandoned, as the media is financed by agenda toting patrons, and beguiled by access to elite circles.
So egregious have the lies and betrayals been that even medical post mortems have been restricted so that deaths could be certified as COVID, amidst multiple comorbidities even in care homes without any formal diagnosis by a doctor. In Europe and the US, we have seen a campaign of psychological terror with misleading stats marinated by behavioral psychologists gleefully disseminated by mainstream media puppets. All roads led to ‘vaccines’ and boosters. Thousands of avoidable deaths were apparently not too high a price to pay to denigrate cheap, proven interventions such as Ivermectin and HCQ.
And with recurring ‘vaccine’ failure the ultimate irony is that once jubilantly ‘vaxxed’ people suddenly found themselves classified as “unvaccinated” requiring regular boosters, all the assurances given to them earlier debased for profit.
Orwell must be aghast at his prophetic prowess. “Democracy” means following orders. It’s not “coercion” but if you don’t comply, we lock you up, fine you and keep you from working if you don’t follow our dictates. And who endowed us with this power? Oh, it’s for the “common good” as asserted by us.
And the new talking points emerge, curiously in tandem. Trudeau asserts that “unvaccinated” are likely racists and misogynists, for daring to prize their physical bodily autonomy. Macron in France says this same constituency are “not really citizens”, thus spake the nutcase whose platform is funded in part by the tax dollars of some of these same “non-citizens.” And a grown man, leading a key European state, says he wishes to “piss them off.” The return of Robespierre? Oh, and Boris, who at least didn’t capitulate over Christmas/New Year feels obligated to intone any disagreement is “mumbo jumbo”. Apparently, that’s the case even if coming from the world’s leading researchers and epidemiologists or corroborated by the success of “low vax” Africa (less than 6% vaccinated) or the fast Omicron rebound of South Africa (27% roughly “vaccinated”). Oh, we should all aspire to the calamities and civil rights cacophonies of Europe (those attack dogs and batons were inspiring to every humanitarian surely at the recent protests in Amsterdam), with some of the worst results in the world in terms of “cases” and “mortality.”
So, time for us, to detach from the “mainstream”, lest we end up babbling nonsense like Supreme Court Justices in the US showcasing truly invincible ignorance. Lies are streaming incessantly. Time to take the reins of our own education. And when a gaggle of “leaders” start spewing divisive, unscientific nonsense, let’s listen to the guidance given by freedom fighters of old with highly contemporary resonance…don’t let the lies pass through you. Time to stand up and speak up and reclaim both sanity and civilization.
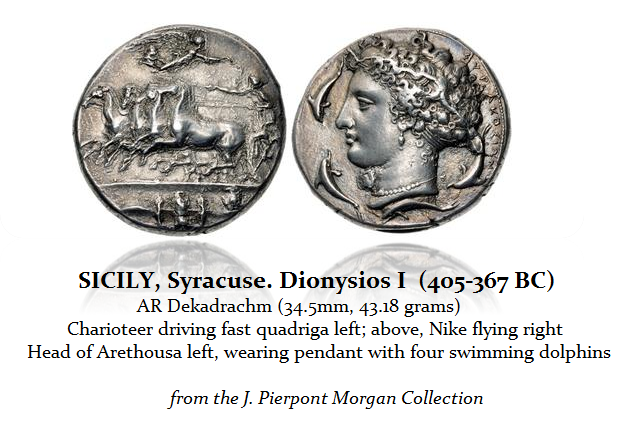
The annual New York Coin show auctions set some unbelievable records this year. This beautiful Dekadrachm of Syracuse which last year would have sold for $50,000, brought $132,000. Another Dekadrachm signed by the artist Kimon estimated at $60,000 sold for $252,000. Granted, this was a famous coin that was part of the J.P. Morgan collection of ancient coins at CNG’s XXV Auction.
This denarius of Quintus Labienus Parthicus brought $150,000 which would have brought $35,000 10 years ago. Then there was one of two known Mark Antony legionary denarius noting Legion XXXII brought $62,400 on a $2,000 estimate. A simple bronze coin of Phoenicia with Mark Antony and Cleopatra estimated at $1,500 sold for $24,000. Many coins appear to have sold up about 50% from the previous year.
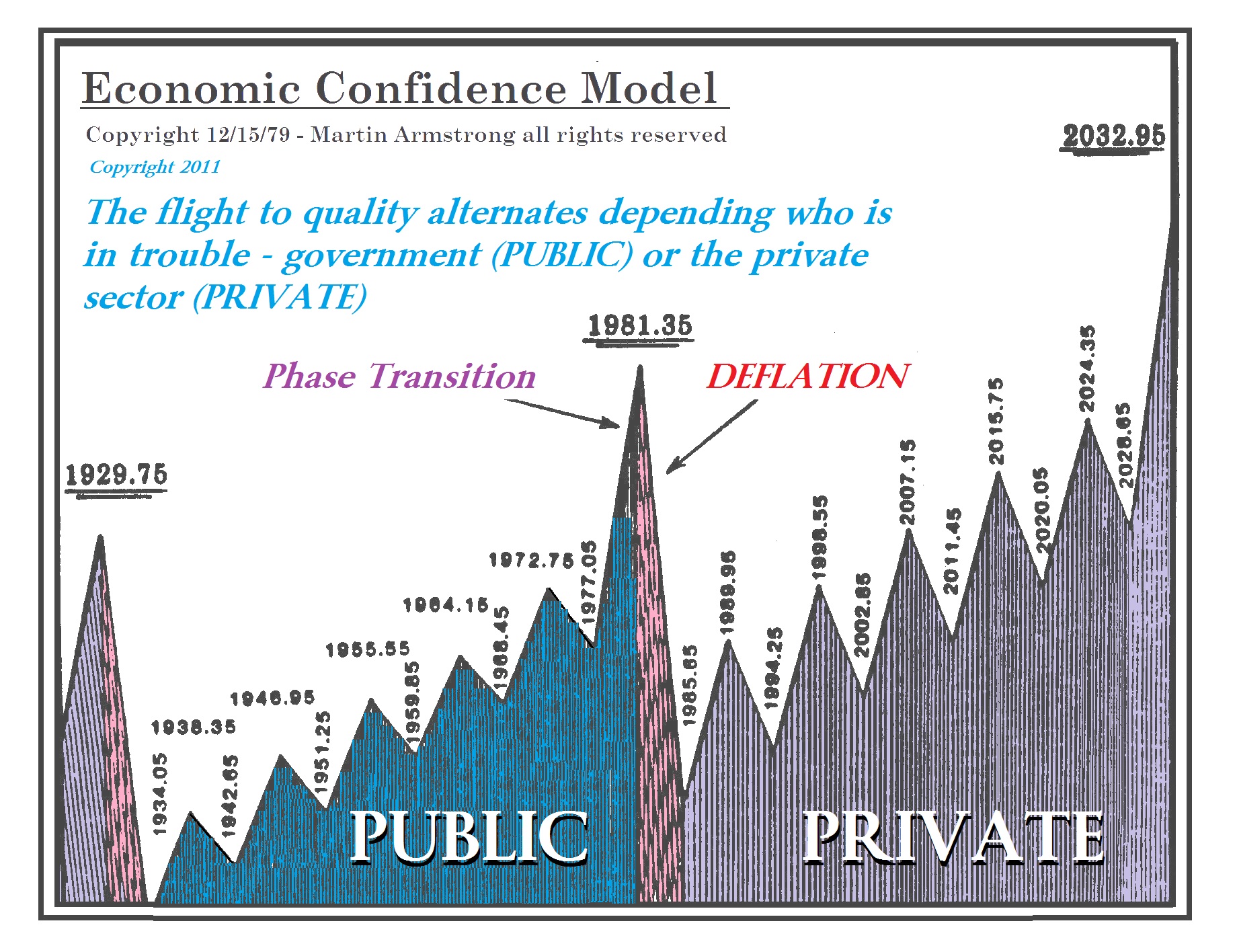
The dollar has clearly peaked in terms of purchasing power given that all tangible assets are rising from collectibles, antique cars, art, real estate, and even comic books. This appears to be part of the entire shift from Public to Private with respect to confidence is concerned. This is a Private Wave that will peak in 2032 with the collapse in confidence of government; Biden and the rest of the COVID nonsense are doing a great job at that. The previous Private Wave peak in 1929.75 followed by the Great Depression and political change by 1934. The same will be true come 2032-2037.
I have created this site to help people have fun in the kitchen. I write about enjoying life both in and out of my kitchen. Life is short! Make the most of it and enjoy!
This is a library of News Events not reported by the Main Stream Media documenting & connecting the dots on How the Obama Marxist Liberal agenda is destroying America