US District Judge Kathryn Kimball Mizelle has determined that the US Centers for Disease Control and Prevention (CDC) violated the law by forcing travelers to wear masks — there is no longer a mask mandate for US travel. The ruling first went into effect in February 2021, and despite declining cases, the health agency and Biden Administration refused to lift the mandate. And the CDC continually pushed back its deadline without providing a clear reason. The judge determined “the mandate exceeded the CDC’s statutory authority, improperly invoked the food cause exception to notice and comment rulemaking, and failed to adequately explain decisions.”
Furthermore, the CDC overstepped bounds by placing a mandate on personal behavior rather than “cleaning measure,” which is under their authority. It was not until this pandemic that the CDC was granted dictatorship powers over our lives. Mizelle also pointed out that although the CDC requires masks for travel, they do not have a mandate in place for anywhere else in America. The “science” does not add up.
Since the ruling, nearly all airlines have dropped mask requirements. Amtrack said that masks are no longer required on trains. Uber, Lyft, and rideshare programs have dropped the mandate. The TSA is no longer enforcing mask mandates at airports – a touch of normalcy is in the air.
However, Biden could still fight the ruling. With his bottom-of-the-barrel approval rating, it would be political suicide. Secretary Psaki last said she is “disappointed” with the ruling (i.e., loss of control) and that the Biden Administration is still urging everyone to normalize covering their faces with fabric for no valid reason.
Posted Originally on the conservative tree house on April 19, 2022 | sundance
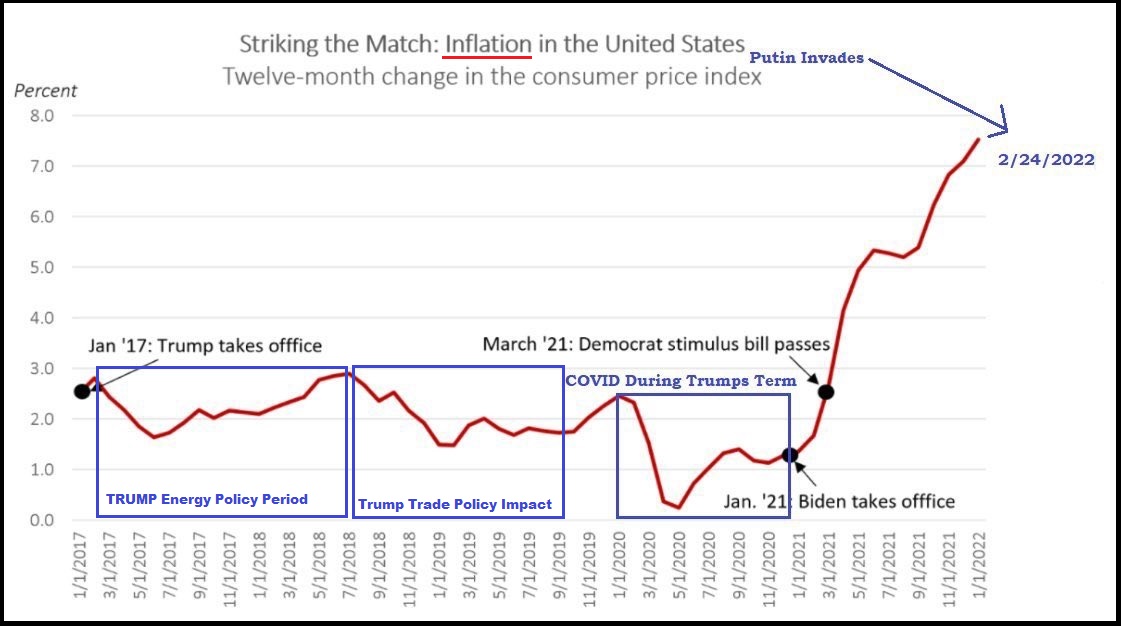
Lots of people talk about an inflation driven recession. Essentially, that’s a total economic contraction in the value of goods and services produced, sold and purchased, due to rising prices. However, as CTH has been pointing out for more than six months, if you subtract the federal COVID infusion money from the overall economy, we have been in a contracting demand economy for almost nine months.
A negative GDP outcome is quite possible, perhaps likely, when the first quarter GDP figures are released on the last Friday of this month. The most recent sales and economic data shows that U.S. consumers are prioritizing spending and high priced durable good sales are negative.
Now, Fannie Mae is delivering a rather stunning shift in their economic forecast. In addition to projecting a recession for 2023, these revised home purchase figures are remarkable:
...”We have downgraded our total home sales forecast for 2022 to a decline of 7.4 percent (previously a 4.1 percent decline) followed by a decrease of 9.7 percent in 2023 (previously a 2.7 percent decline).” (link)
That is a very significant change in home sales forecast to the negative position.
We already have serious energy inflation to contend with and low wage growth. We already know a third inflation wave on highly consumable goods is coming this summer, likely around 30% or more in food prices at the grocery store.
The professional forecasts are always tilted toward the positive for this administration, so this new statement by Fannie Mae should be considered accordingly. Remember, Boy Scouts motto.
By Matt Walsh originally Published on Rumble on April 18, 2022
Today on the Matt Walsh Show, leftists are fighting passionately to defend the profit margins of the pharmaceutical industry, even as Big Pharma uses an entire generation of children as lab rats. Also, federal officials hunt for the murderer of a dolphin, while letting the murderer of five infant children off the hook. Plus an MSNBC analyst explains why it’s a threat to free speech to allow people to say whatever they want on social media. And a Democrat candidate for congress aborted her child to save the planet. Finally in our daily cancellation, Ilhan Omar is upset because Christians were singing on a plane. We’ll talk about all of that and more today on the Matt Walsh Show.
NBA star Jonathan Isaac has withstood immense pressure to conform to popular social issues. He’s now writing a book about his experience and is publishing with the Daily Wire. Pre-order your copy now: https://utm.io/ud96e.
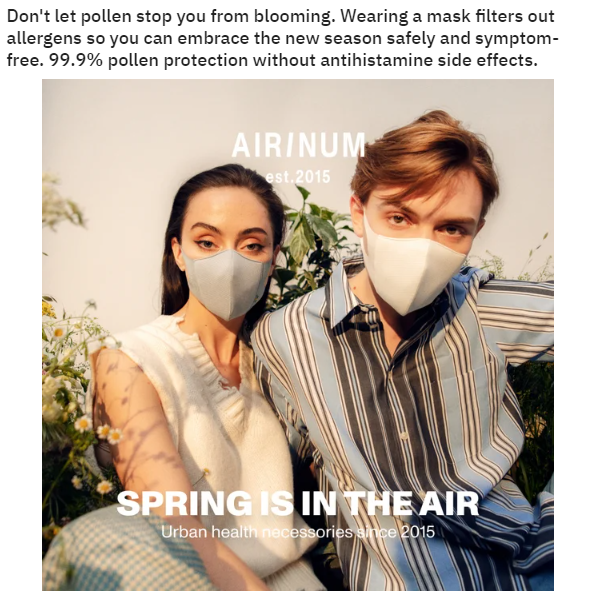
The attempt to normalize wearing masks is in full swing. “Don’t let pollen stop you from blooming,” the advertisement states as if the public avoided seasonal changes before masks became widely available. Covering half of your face is not normal in our Western society. A portion of the population is still afraid to breathe in the fresh air and craves a reason to muzzle the masses once again. As a reminder, the Centers for Disease Control and Prevention admitted that cloth masks are ineffective.
In an even more pathetic attempt to normalize masks, “studies” find that people seem more attractive when wearing a mask. If covering half of your face makes you more attractive, you’re simply ugly by today’s beauty standards. It is better to look ugly rather than ugly and stupid.
Posted originally on the conservative tree house on April 13, 2022 | Sundance
The CDC announced today {SEE HERE} they are extending the federal emergency order requiring masks on planes, trains and public transportation for a period of 15 days, ending May 3rd.
The mask mandate was set to expire April 18. However, the Biden administration will keep the requirement in place for another 15 days under the justification of a rise in COVID-19 cases driven by the new BA.2 sublineage of the Omicron variant.
(Press Release) – […] The CDC Mask Order remains in effect while CDC assesses the potential impact of the rise of cases on severe disease, including hospitalizations and deaths, and healthcare system capacity. TSA will extend the security directive and emergency amendment for 15 days, through May 3, 2022. (link)
There are contradicting claims on the benefits and/or futility of wearing masks to avoid spreading the COVID-19 virus. Several scientific studies have found no significant benefit; however, the theatrics of mask wearing is now a litmus test for global virtue.
Philadelphia, Pennsylvania, has recently announced a new indoor mask mandate for their extended metropolitan area. Fauci soundbite below.
TrialSite chronicled the efforts of Dr. Jackie Stone in Zimbabwe during the worst stages of the pandemic. Born in Zimbabwe, Dr. Stone has been fascinated by research since a young age, and her commitment to caring for people during the pandemic has been legendary. While her off-label ivermectin-based combination regimen was identified with the saving of many lives in this southern African country, the medical establishment isn’t too keen on thinking outside of the box, even during the worst pandemic in a century. Dr. Stone now faces a court trial with criminal charges for merely treating COVID-19 patients with an early outpatient treatment protocol based on a combination of off-label treatments that includes ivermectin. This, even though Dr. Stone treated many in the Zimbabwe government and military successfully. In fact, for a while, the Medicines Control Authority of Zimbabwe (MCAZ) authorized access on an emergency basis for research—which amounted to care in this low-and middle-income country. The regulatory agency did a turnaround with ivermectin due to the results in the clinic of Dr. Jackie Stone.
Articles about Dr. Stone and Zimbabwe can be found at TrialSite. A fighter to the end originally of English and Norwegian descent, curious, and tough, yet elegant and empathetic, she grew up in the bush in this part of Africa, as her father was involved with geology and mining. Dr. Stone’s ethos, integrity, and commitment to doing good should have led her to awards from groups such as the World Health Organization.
Together Trial Mainstream Media Interpretations Could Put Low-Cost Regimen at Risk in MICs
Stone recently got together remotely with TrialSite’s founder Daniel O’Connor to discuss her concern with the Together Trial. While mainstream media have pounced on the findings, at least a dozen physicians and scientists are findings various issues with the data.
Ed Mills, the principal investigator, did the right thing investing his time as well as raising money to study repurposed drugs. While the Together trial’s primary endpoint failed to show efficacy for ivermectin, even Mills went on the record in a private email declaring ivermectin proponents should be upbeat about some of the data generated in the study. But Mills’ data was taken by mainstream media and used as a weapon to attack the use of the drug worldwide. This isn’t Dr. Mills’ fault–again he took the time to investigate the drug as well as other important repurposed drugs.
But Stone’s concern centers on the needs of low and middle-income countries (LMICs) for low-cost, available regimens for early care. Stone told TrialSite, “in poor and up-and-coming countries we don’t always have the luxury of waiting around for gold standard evidence. Rather, in the case of the pandemic, we need to move fast, and we did, leading to the saving of many thousands of lives.”
She continued, “My concern now is that papers such as the New York Times or Wall Street Journal pounce on data, often misinterpreting quotes from the PI can lead to a cutting off of life-saving approaches in LMICs such as my country.”
“Dr. Stone’s commitment to LMICs cannot be denied based on a clear track record of success. With COVID-19 came politics around the use of off-label drugs such as ivermectin, and unfortunately, Dr. Stone is caught in the middle of a political battle, but she is one of the most resilient individuals I have ever come across,” reports TrialSite’s O’Connor.
What about Together?
Dozens of scientists and doctors now pour through data of the Together Trial. Recently, Dr. David Wiseman, affiliated with TrialSite, shared a dozen bullet points of concern associated with Together, including inputs from Dr. Flavio Cadegiani and others that TrialSite poses as questions.
Together Trial Questions: Ivermectin
#
Question/Concern Issues for Discussion with Together Trial
1.
Did the ivermectin arm of Together run later than the placebo arm, a time when a more virulent strain was present in that part of Brazil?
2.
Why wouldn’t the protocol call for screening for ivermectin use—after all the drug was used in many parts of Brazil. Were those participating already using the drug? It would be hard to prove now.
3.
The critics fret about the lack of reported boosts in gastrointestinal side effects in the ivermectin arm leading to what they believe is a fundamental problem with the study—either A) placebo group was on ivermectin or B) those taking ivermectin were not administered real study drug
4.
Were these placebo pills produced to look identical to the study drug? As the drug is commonly used, this would have unblinded the study.
5.
Together used ivermectin alone yet the early care community uses the drug in combination with other economical safe drugs such as antibiotics, steroids, as well as nutraceuticals such as vitamin D, C, and zinc. The study of ivermectin alone doesn’t mean much to frontline doctors.
6.
Together started up to 8 days post symptom onset, but frontline ivermectin proponents declare the drug should be given immediately upon symptomatic infection. The P.1 variant also saw a faster progression to severe illness only compounding the problem.
7.
In the Together study, they used a dose of (0.4 mg per kilo per day) which many critics called inadequate for ill patents–was the study underdosed?
8.
Given ivermectin proponents suggest using the drug till symptoms are resolved, why did the Together protocol only call for use for 3 days?
9.
Why did the protocol call for administration of the drug on an empty stomach when proponents declare the drug works best when associated with consumption of fatty food?
10.
Why is so much basic data missing from the study results such as Recruitment Period, Recruitment Locations, Recruitment and allocation order per sit, Description of how the molecules and placebo were produced or compounded to look identical (otherwise loss of blinding); why is there missing age data for 98 patients? Other gaps in data or anomalies are present for those interested
11.
Some basic math shows that the numbers listed in the trial paper for the different arms and outcomes in the trial do not add up to the totals and percentages that they give – either a gross mathematical error or fraud. To see many of the strange mathematical discrepancies which invalidate the trial conclusions, go to investigative journalist Phil Harper’s article: Moreover Wiseman declares And the alteration of the death count in the trial data raises serious questions:
Seeking more information about Dr. Stone?
For all of those interested in Dr. Stone’s story check out the many articles published in TrialSite along with this important letter authored by Dr. Eleftherios Gkioulekas, Professor of Mathematics Undergraduate Program Coordinator at The University of Texas — Rio Grande Valley School of Mathematical and Statistical Sciences in Edinburg, Texas.
Call to Action: TrialSite suggests a fund to support Dr. Stone in her legal battle if needed.
Recently scientists from Denmark led an important study suggesting that mRNA-based vaccines such as the ones made by Pfizer or Moderna may not be as safe as adenovirus-based vaccines such as Johnson and Johnson, AstraZeneca/Oxford or the one produced by China’s CanSino Biologics. Led by Peter Aaby, a trained physician and anthropologist that runs a health and demographic surveillance system site in West Africa as part of the Bandim Health Project and Dr. Mihai Netea a well-known award winning Romanian/Dutch scientists and Danish colleagues from Odense Patient Data Explorative Network (OPEN) at University of Southern Denmark, the group scrutinized possible “non-specific effects” (NSEs) of the COVID-19 vaccines probing into overall mortality such as not only COVID-19 deaths but also accidental deaths, cardiovascular deaths and other non-COVID-19 deaths. The team discovered that out of 74,193 participants in mRNA clinical trials and 61 deaths, that based on relative risk there was no real difference between the vaccine and placebo group. While in the adenovirus-based studies with 122,164 participants and 46 deaths the vaccine had nearly half the level of deaths as compared to the controls group.
The study team decided to take a step back and look at the COVID-19 vaccine clinical trial data from a different point of view. They did this because “there is now ample evidence that vaccines can have broad heterologous effects on the immune system.” Such effects can either A) greater protection or B) increased susceptibility to unrelated infections or even other non-infectious autoimmune diseases. The authors report that emerging study data reveals that “vaccines may have completely unexpected effects on overall mortality, different from what could be anticipated based on the protection against the vaccine-targeted disease.”
The study results await peer review thus the data shouldn’t be considered evidence. But the novel approach and consequent findings represent an important potential contribution to our scientific knowledge of the COVID-19 vaccines.
Overall Mortality wasn’t Studied
Taking a different perspective, Dr. Aaby and team share that the current batch of COVID-19 vaccines were not tested to evaluate their effects on overall mortality. That would have been difficult given the short follow-up in the studies as subjects participating in the control groups received the vaccine after 3-6 months based on the emergency use authorization situation.
Surprisingly, although all would assume that the COVID-19 vaccines would reduce overall mortality in the pandemic this assumption hasn’t been formally vetted in studies.
The authors utilized the final study reports available from the COVID-19 vaccine trials investigating the impact of mRNA and adenovirus-vector COVID-19 vaccines on overall mortality, including the previously mentioned other categories such as cardiovascular-related deaths.
The Findings
The table below highlights these study findings:
Participants
Deaths
Relative Risk
mRNA
74,193
61 (mRNA 31; placebo; 30)
1.03 (95% CI=0.63-1.71)
Adenovirus
122,164
46 (vaccine: 16; controls:30)
0.37 (0.19-0.70)
Aaby and team report that the adenovirus-vector vaccines were associated with protection against COVID-19 deaths (RR=0.11 (0.02-0.87)) and non-accident, non-COVID-19 deaths (RR=0.38 (0.17-0.88)).
Of note, mRNA-based vaccines differ markedly from adenovirus vaccines regarding impact on overall mortality (p=0.030) as well as non-accident, non-COVID-19 deaths (p=0.046). The placebo-controlled RCTs of COVID-19 vaccines were halted rapidly due to clear effects on COVID-19 infections. Importantly the data derived from this study suggest an important need for randomized controlled trials of mRNA and adeno-vectored vaccines head-to-head comparing long-term effects on overall mortality.
Brief Discussion
Of course, many experts may summarily dismiss such findings as not relevant. After all the COVID-19 studies were designed to determine if the vaccines were effective in protecting against death from SARS-CoV-2, the virus behind COVID-19. Yet the authors point out that “non-specific effects, and their immunological basis, have been established for several other vaccines.” For example, the authors point to randomized controlled trials showing that BCG vaccine against tuberculosis (TB) lessens neonatal mortality, yet this was because the vaccine protects against deaths from sepsis and respiratory infections.
They point out that “immunological studies have shown that such effects are indeed biologically plausible; BCG positively affects the innate immune system leading to enhanced resistance towards a broad range of pathogens. Furthermore, the BCG vaccine has been associated with decreased systemic inflammation.”
Conclusion
The authors conclude that if their findings are in fact validated by randomized controlled studies then the adenovirus-based vaccines may prove beneficial to their “protective heterologous effects…on non-COVID-19 mortality” as well as their effectiveness against SARS-CoV-2 infection. Could these vaccines represent an advantage in vulnerable populations susceptible to cardiovascular mortality. Key is a better understanding of the heterologous effects between the different vaccine types.
Study Funding
Dr. Allen Schapira funded the work on non-specific effects of vaccines while some of the previous work was funded by the Danish Council for Development Research, Ministry of Foreign Affairs, Denmark; Novo Nordisk Foundation and European Union.
Lead Research/Investigator
Peter Aaby, DMSc, Bandim Health Project, INDEPTH Network; Bandim Health Institute – OPEN, Institute of Clinical Research
Christine Stabell Benn, University of Southern Denmark – Odense Patient Data Explorative Network (OPEN); Bandim Health Project, INDEPTH Network
Sebastian Nielsen, University of Southern Denmark – Odense Patient Data Explorative Network (OPEN)
Mihai G. Netea, Radboud University Nijmegen – Radboud Center for Infectious Diseases (RCI); Radboud University Nijmegen – Department of Internal Medicine
Florida Governor Ron DeSantis has proven time and time again that he is a man of the people. DeSantis signed SB 988, the No Patient Left Alone Act, which guarantees that no one in the state of Florida will be left to die alone in hospitals, hospices, and long-term care facilities. Under the tyrannical COVID laws, countless people were unable to see their loved ones during their final days. This is a malicious and deliberate attempt to force the population to cave to Big Pharma as the medical community can no longer deny that the vaccination does not prevent transmission.
Numerous states still require proof of vaccination or a PCR test to enter medical facilities. A friend of mine recently lost her grandfather, and her 90-year-old grandmother was prohibited from entering the New York-based facility as she was not vaccinated. The PCR results take time to process and are only valid for a few days. There were no final words or hugs goodbye. These laws have deeply punished everyone in our society.
DeSantis is finally putting an end to this unfounded oppression. “Throughout the pandemic, the federal government has waived protections for families to visit their loved ones in hospitals and long-term care facilities. That is unacceptable,” said Governor Ron DeSantis. “Here in Florida, we recognize that family and human connection is one of the most important aspects of physical, mental, and emotional well-being and we are ensuring Floridians are never again denied the right to see their relatives and friends while in hospitals or nursing homes.”
The new law will protect families and loved ones facing the most painful of circumstances:
End-of-life situations.
A resident, client, or patient who was living with family before being admitted to the provider’s care is struggling with the change in environment and lack of in-person family support.
A resident, client, or patient is making one or more major medical decisions.
A resident, client, or patient is experiencing emotional distress or grieving the loss of a friend or family member who recently died.
A resident, client, or patient needs cueing or encouragement to eat or drink which was previously provided by a family member or caregiver.
A resident, client, or patient who used to talk and interact with others is seldom speaking.
For hospitals, childbirth, including labor and delivery.
Pediatric patients.
Indeed, the system has also deserted “pediatric patients” due to these unfathomable restrictions. “The No Patient Left Alone Act is about protecting human dignity and compassion,” said Senator Ileana Garcia. This should be protected as a fundamental human right. I do not see this becoming a Federal-level ruling as the Biden Administration wants dissenters to suffer.
People are starving in Shanghai. The screams heard in the disturbing video above are due to more than mere frustration. China placed millions under a strict lockdown that was initially supposed to last for five days. As cases allegedly spread, China extended the lockdown indefinitely under their zero-COVID tolerance policy.
Those who prepared for a five-day lockdown are now rationing what food and water they have left. The tap water is not necessarily safe for consumption, and people have begun to boil water if they have the means to do so. According to my sources, people living within communities rally together to buy bulk food orders when possible for a premium. China is offering a closed-loop system for some workers, who must live at their job site for the remainder of the lockdown. Therefore, workers are in short supply, and demand is extremely high. Hungry citizens typically log on to food delivery apps early in the morning and usually only have a few minutes to place their bulk orders. The food they receive is carefully rationed as the next meal is not guaranteed.
The barter system always emerges in times of disaster. People are trading with one another where possible, although they are forbidden from actually leaving their residences. No one is permitted to visit relatives or check on the elderly or disabled. Worse, people are unable to access medical care or prescription drugs. The government continues to provide rationed food, but its rollout has been so ineffective that most simply do not have access to food.
China will allow its people to die from dehydration and starvation to protect them from a virus with a negligible death rate. This is how revolutions begin.
I have created this site to help people have fun in the kitchen. I write about enjoying life both in and out of my kitchen. Life is short! Make the most of it and enjoy!
This is a library of News Events not reported by the Main Stream Media documenting & connecting the dots on How the Obama Marxist Liberal agenda is destroying America